
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-187
Transcatheter Closure of Coronary Cameral Fistula From Right Coronary Artery to Right Atrium With Cocoon Patent Ductus Arteriosus Device
By Polavith Chutisira, Vorarit Lertsuwunseri, Siriporn Athisakul, Suchat Sricholwattana, Suphot Srimahachota
Presenter
Polavith Chutisira
Authors
Polavith Chutisira1, Vorarit Lertsuwunseri1, Siriporn Athisakul2, Suchat Sricholwattana3, Suphot Srimahachota1
Affiliation
King Chulalongkorn Memorial Hospital, Thailand1, Kcmh, Thailand2, HRH Maha Chakri Sirindhorn Medical Center, Thailand3,
View Study Report
TCTAP C-187
STRUCTURAL HEART DISEASE - Others (Structural Heart Disease)
Transcatheter Closure of Coronary Cameral Fistula From Right Coronary Artery to Right Atrium With Cocoon Patent Ductus Arteriosus Device
Polavith Chutisira1, Vorarit Lertsuwunseri1, Siriporn Athisakul2, Suchat Sricholwattana3, Suphot Srimahachota1
King Chulalongkorn Memorial Hospital, Thailand1, Kcmh, Thailand2, HRH Maha Chakri Sirindhorn Medical Center, Thailand3,
Clinical Information
Patient initials or Identifier Number
S.S.
Relevant Clinical History and Physical Exam
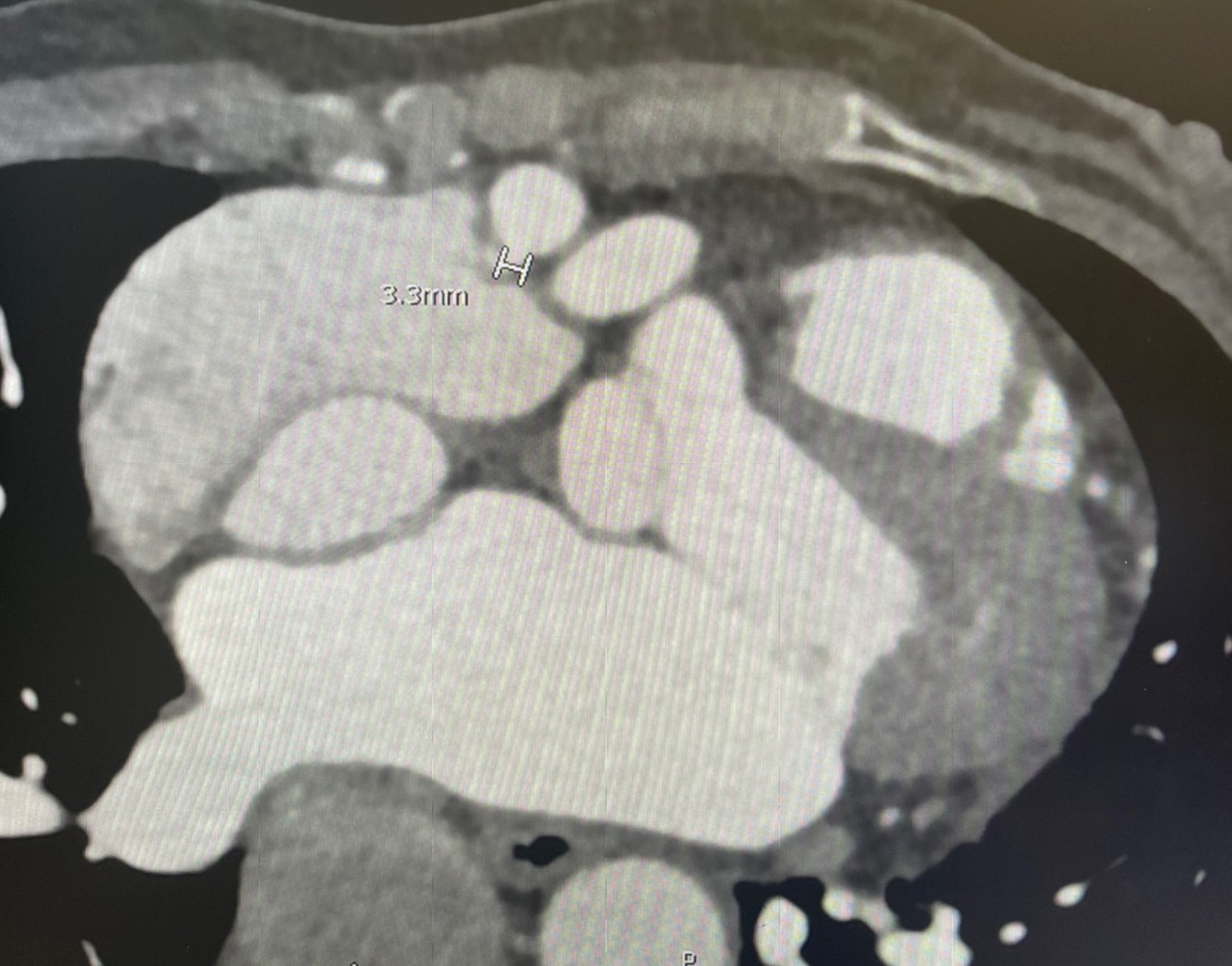
A 58-year-old male presented with dyspnea on exertion without any chest pain. His only underlying disease was hyperlipidemia. He was investigated with coronary computed tomographic angiography (coronary CTA). The result showed no significant stenosis of the coronary arteries but demonstrated tortuosity and aneurysmal dilatation of the proximal right coronary artery (RCA), size 0.9–1.5 cm in diameter, connected to the right atrium (RA). He was referred for transcatheter device closure.
Relevant Test Results Prior to Catheterization
A 12-lead electrocardiogram showed normal sinus rhythm with frequent premature atrial complexes and left ventricular hypertrophy by voltage criteria.His chest radiograph was unremarkable. Laboratory findings were within normal limits. We reviewed the coronary CTA that the patient had already done, which demonstrated the narrowest diameter of the aneurysmal neck of the fistulous tract at the RA entry side was 3.3 mm (Figure 1).
Relevant Catheterization Findings
Right and left heart cardiac catheterizations were done prior to fistula closure. Hemodynamic findings were normal filling pressures of both ventricles and no pulmonary hypertension. He had oxygen step up from the superior and inferior vena cava (SVC and IVC) to RA level with a left-to-right shunt (Qp:Qs = 1.66).
Interventional Management
Procedural Step
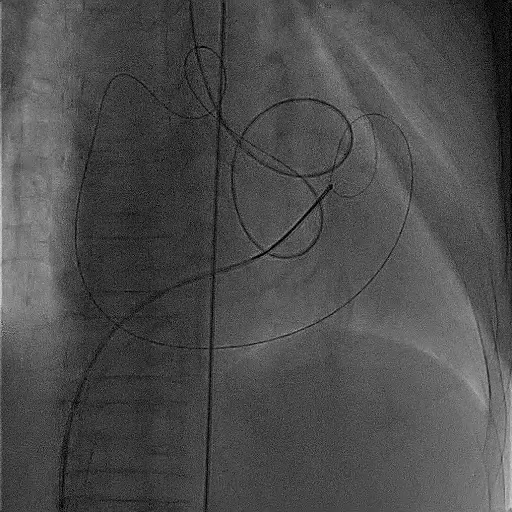
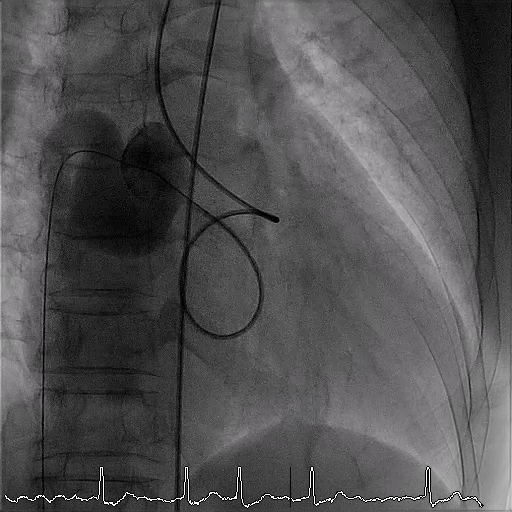
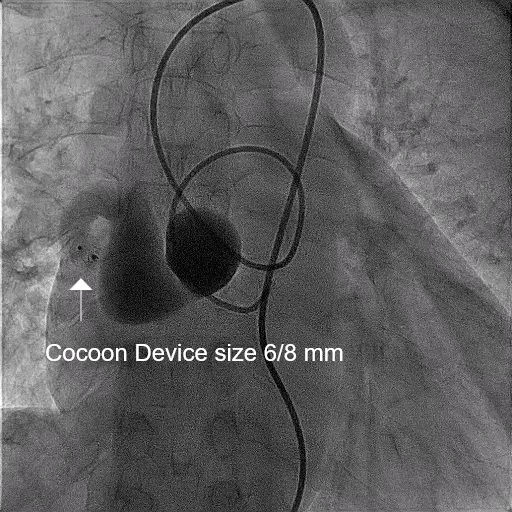
The right femoral vein (RFV) and right femoral artery (RFA) were accessed with a 7-Fr and 6-Fr sheath, respectively. Heparin 3,000 IU was administered intravenously. Judkins Right (JR) 3.5 was inserted with 260 cm, 0.035-inch Terumo guide wire via RFA. We passed the guide wire across the fistulous tract to the RA, right ventricle (RV), and placed at the pulmonary artery (PA). A multipurpose guiding catheter was inserted with a 260-cm, 0.035-inch standard guide wire via RFV and passed to the PA, then exchanged the guidewire for the 10-mm snare catheter for snaring the Terumo guide wire (Figure 2). The AV loop was formed, and the multipurpose guiding catheter was removed. We advanced the JR catheter to the aneurysmal part. Hand-injection with low-osmolar contrast media was done (Figure 3). The narrowest diameter of the RA entry side was 3.2 mm, so a Cocoon patent ductus arteriosus (PDA) device, size 6/8 mm, was chosen for the fistula closure. We exchanged the RFV sheath for the Durasheath and advanced to the fistulous tract from the RA side, then inserted the Cocoon PDA device via the Durasheath and deployed it just ahead of the narrowest part. Angiography via JR showed no contrast leaked to RA, so the Cocoon PDA device was released from the cable. The selective final angiogram after device deployment revealed complete occlusion of the fistula at the RA level (Figure 4).
Case Summary
Coronary artery fistulas are rare coronary anomalies but often lead to clinical sequelae when the size is large enough. Transcatheter fistula closure is the technique with high success rate for closing the fistula. In the fistulous tract with the neck at the entry side, the Cocoon PDA device can be used instead of vascular plugs or embolization coils. The occlusion of the fistula with the Cocoon PDA device is satisfactory, but the outcomes still need long-term follow-up.