
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-101
Rotational Atherectomy in False Lumen Rescued by Retrograde Chronic Total Occlusion Techniques
By Jiunn-Wen Lin, Jih Tze Tan
Presenter
Jih Tze Tan
Authors
Jiunn-Wen Lin1, Jih Tze Tan2
Affiliation
Dalin Tzu-Chi General Hospital, Taiwan1, Dalin Tzu Chi General Hospital, Taiwan2,
View Study Report
TCTAP C-101
CORONARY - Complications (Coronary)
Rotational Atherectomy in False Lumen Rescued by Retrograde Chronic Total Occlusion Techniques
Jiunn-Wen Lin1, Jih Tze Tan2
Dalin Tzu-Chi General Hospital, Taiwan1, Dalin Tzu Chi General Hospital, Taiwan2,
Clinical Information
Patient initials or Identifier Number
W.S.S.
Relevant Clinical History and Physical Exam
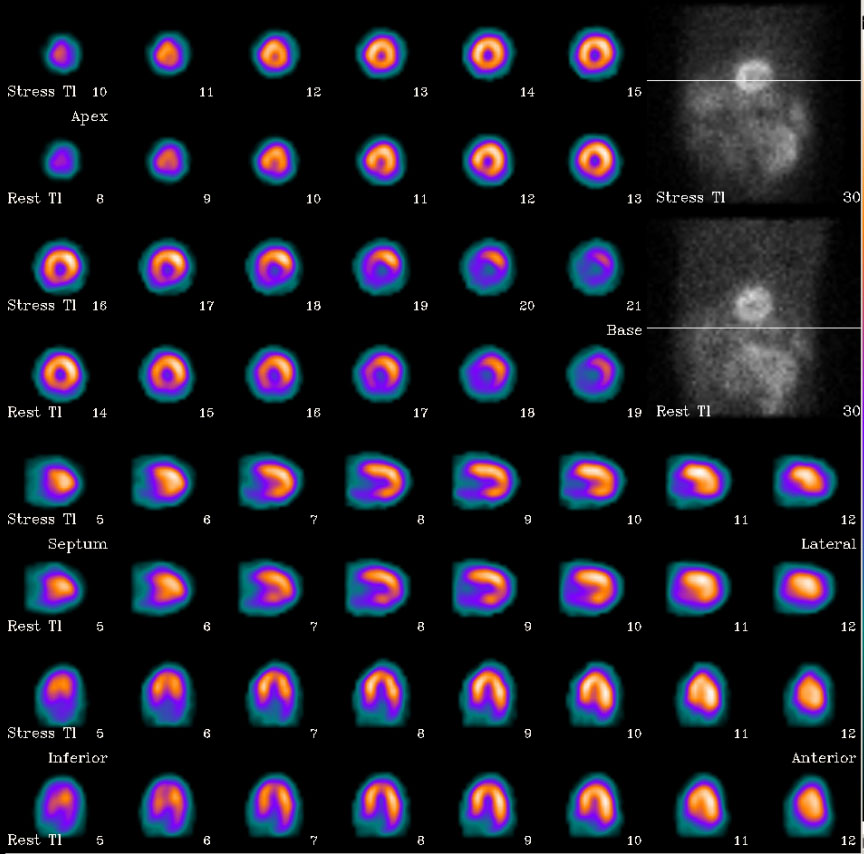
The 62 y/o male with a history of AAA s/p EVAR was admitted to our ward due to effort angina and exertional dyspnea. Thallium201 myocardial perfusion scintigraphy revealed high likelihood for significant stress-induced myocardial ischemia in apical and inferior wall.
Relevant Test Results Prior to Catheterization
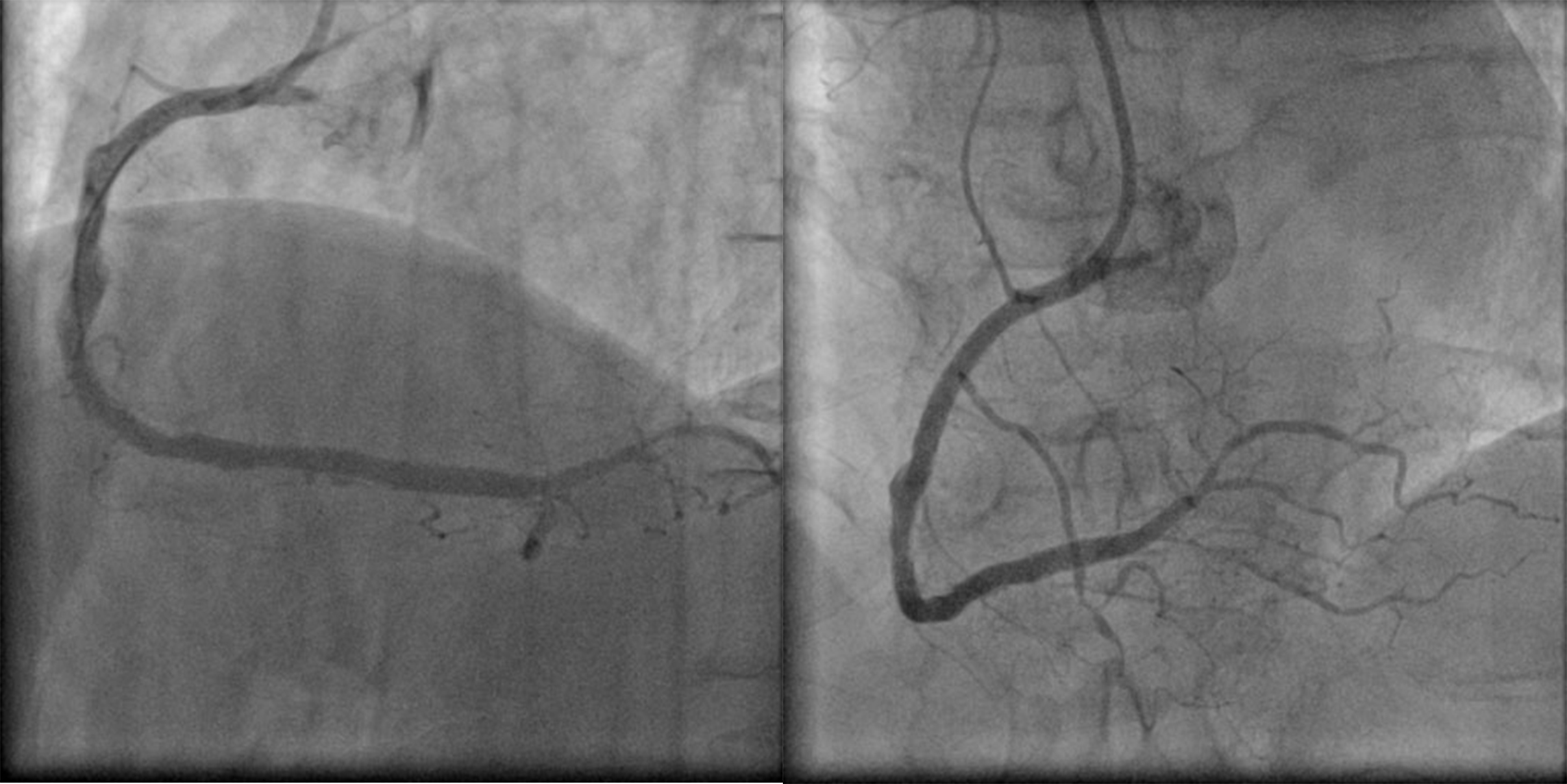
Relevant Catheterization Findings
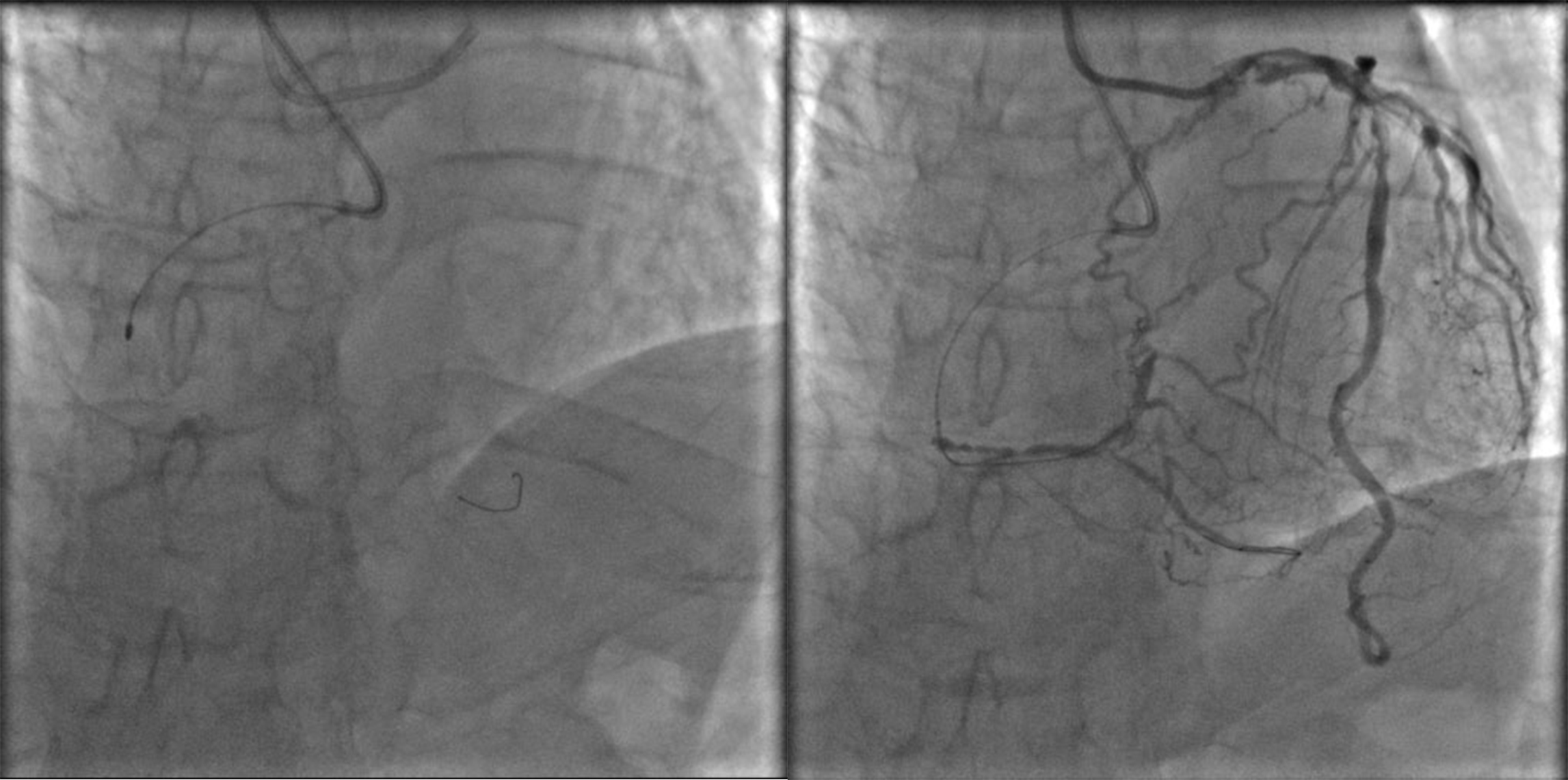
Coronary angiogram revealed significant stenosis in mid-LAD, occluded LCX-OM,and long critical stenosis in mid-RCA. We recommended CABG but the patient declined it. He went to other hospital where PCI for RCA was attempted. The guidewire went into false lumen and subsequently reentered into true lumen at far distal RCA. No device could cross the lesion. Rotational atherectomy was performed entirely in subintimal space after which huge false lumen formed, obstructing distal flow.

Interventional Management
Procedural Step
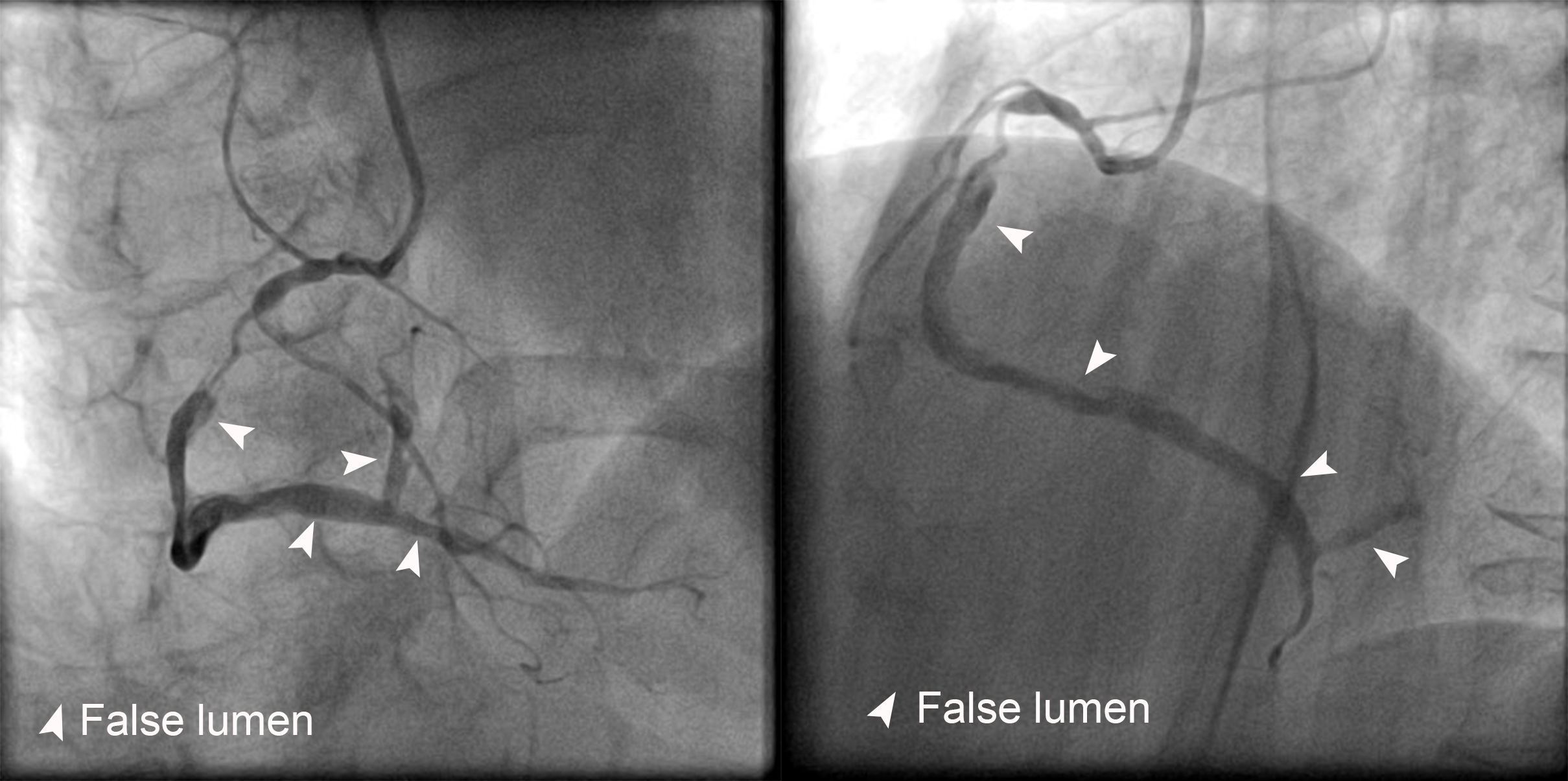
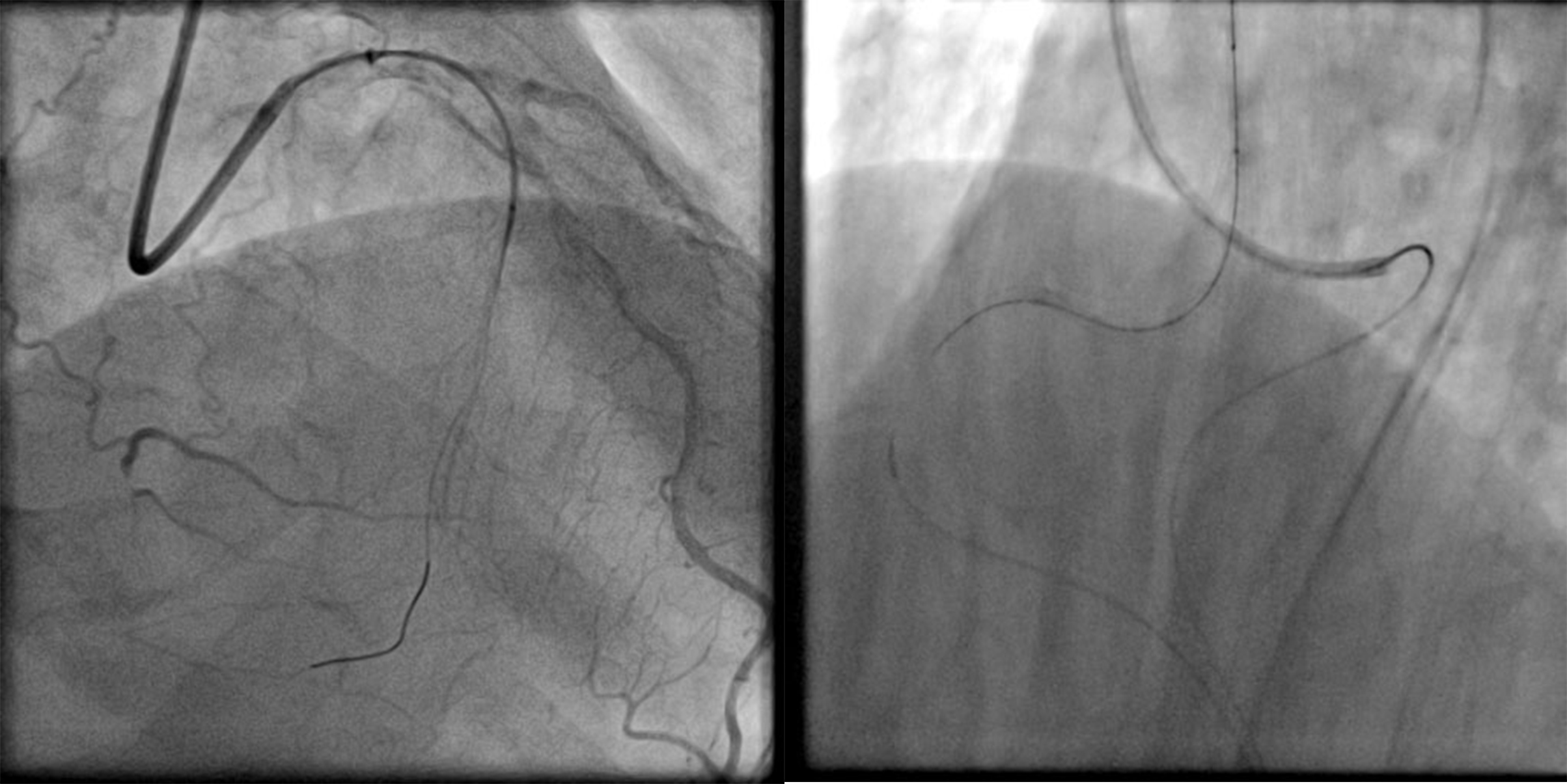
Follow-up coronary angiography revealed huge false lumen from middle RCA to both posterior descending artery (PDA) and posterolateral (PL) branches compressed the true lumen, almost obstructing the antegrade flow. We decided to rescue the situation with retrograde technique.1. We used EBU 3.5 x 7F guiding catheter (Launcher, Medtronic) to engage LM.2. We wired LAD with Sion blue guidewire with support of Corsair microcatheter (Asahi Intecc). On engaging promising septal channel, we changed the guidewire to Sion guidewire (Asahi Intecc) for septal surfing. The Sion guidewire successfully crossed the channel and reached distal RCA. 3. We failed to cross the lesion with Sion guidewire. We tried Fielder XTA guidewire (Asahi Intecc) and crossed the lesion from retrograde direction. Fielder XTA guidewire failed to go into the antegrade SAL 1.0x6F guider. We introduced Guideliner catheter into proximal RCA and manipulated retrograde Fielder XTA into Guideliner and into the antegrade guider. 4.By trapping retrograde guidewire with a 2.5x20 mm balloon, Corsair microcatheter could go through CTO segment into the antegrade guider. We exchanged guidewire to RG3 guidewire for externalization. 5. We dilated the CTO lesion with a 2.0x20 mm balloon at 10 atm. After balloon dilatation, the true lumen came out !6. From distal to proximal, three drug-eluting stents (2.5x38 mm, 2.75x38 mm stent, and 3.0x38 mm) were deployed to scaffold the lesion. Final angiogram was good with TIMI 3 flow.
Case Summary
False lumen created by rotablation may not heal but expand, further compressing the true lumen and compromising distal flow. Rotablation should not be done in long subintima space. The true lumen could be rescued by retrograde CTO techniques even after weeks of external compression of long and huge false lumen.