
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-043
Orbital-Tripsy in Calcified Ostial Lesion
By Jonathan Gabriel Sung
Presenter
Jonathan Gabriel Sung
Authors
Jonathan Gabriel Sung1
Affiliation
Tuen Mun Hospital, Hong Kong, China1,
View Study Report
TCTAP C-043
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Orbital-Tripsy in Calcified Ostial Lesion
Jonathan Gabriel Sung1
Tuen Mun Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
YSM
Relevant Clinical History and Physical Exam
We report an 85-year-old lady with history of hypertension. She developed acute myocardial infarction complicating an episode of severe pneumonia during which she required mechanical ventilation and ICU care.
Relevant Test Results Prior to Catheterization
Echocardiogram showed dilated LA, LVEF 65%, mild apical hypokinesis, mildly calcified MV with moderate MR, mildly calcified aortic valve with mild AR, no AS, mild TR and no pericardial effusion.
Relevant Catheterization Findings
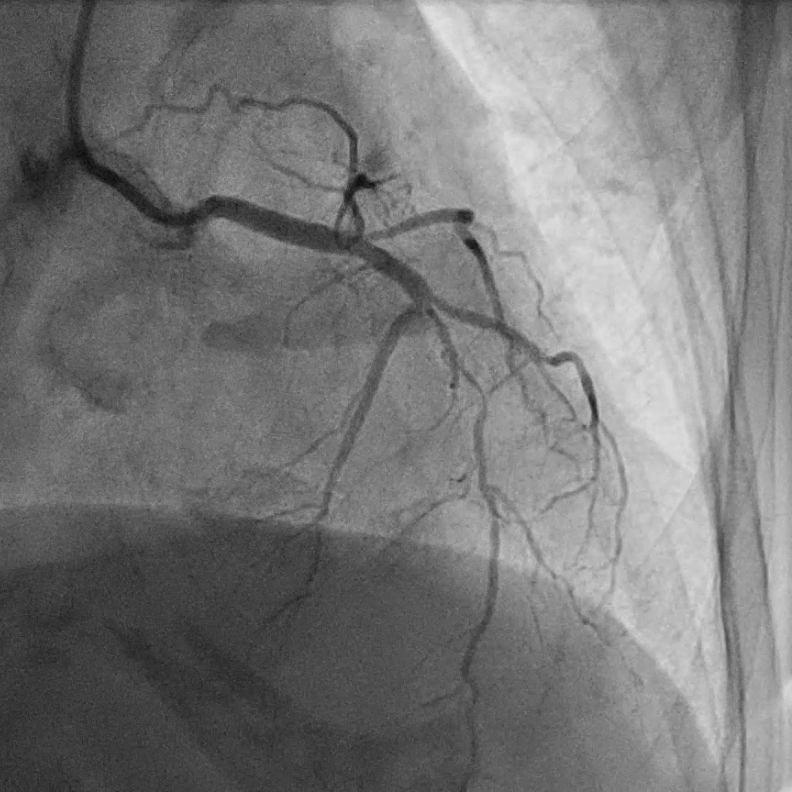
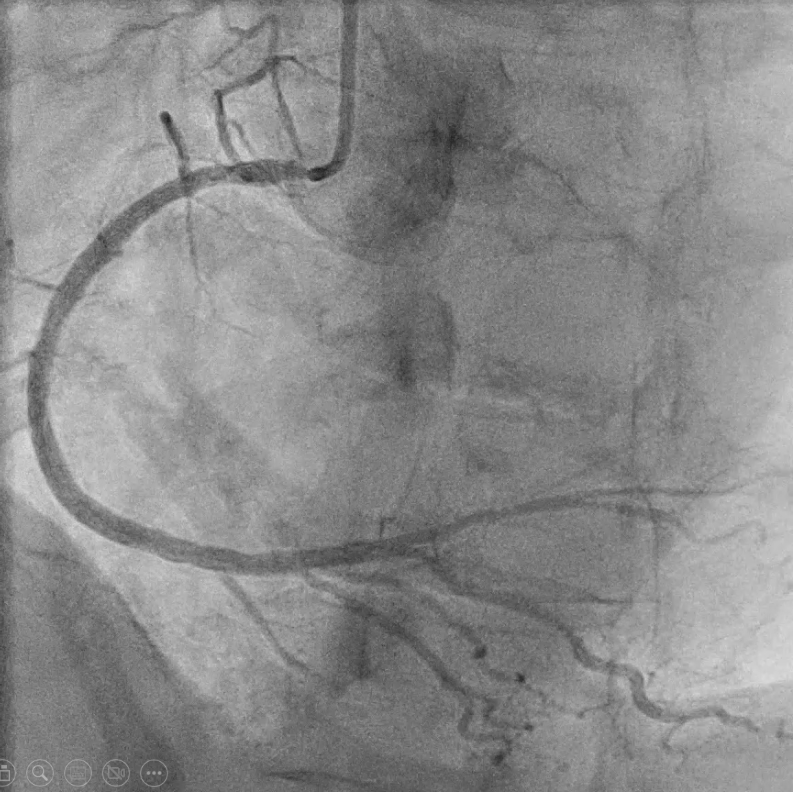
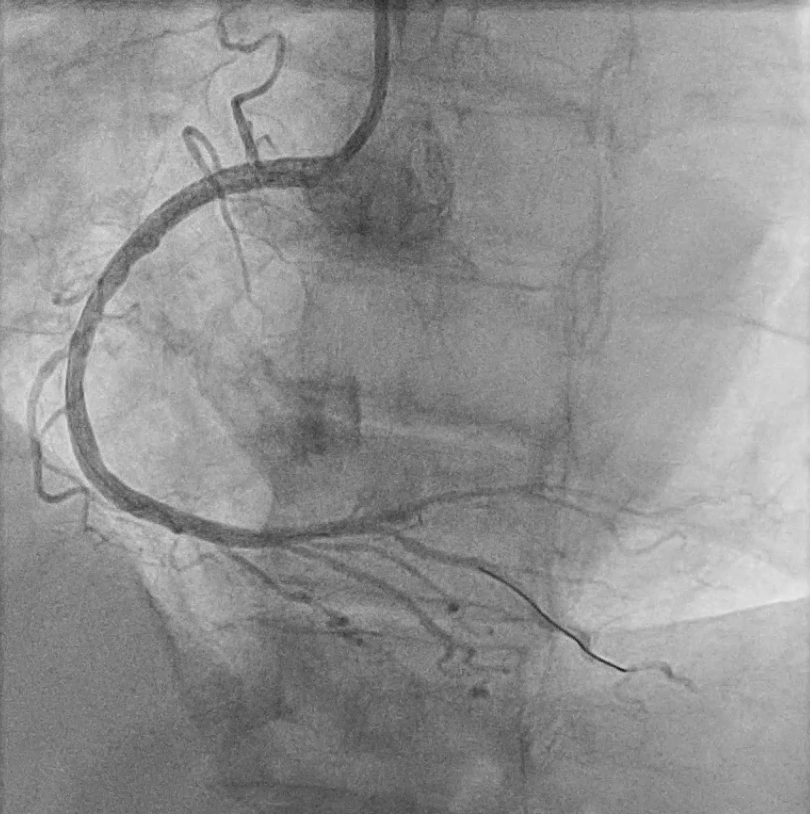
LMS: normalLAD: m-dLAD diffuse severe stenosis up to 95%, ostial D1 70% stenosisLCX: small and non-dominantRCA: pressure damping upon engagement, ostial RCA 80% stenosis, mRCA 40% stenosis, PL moderate stenosis
Interventional Management
Procedural Step
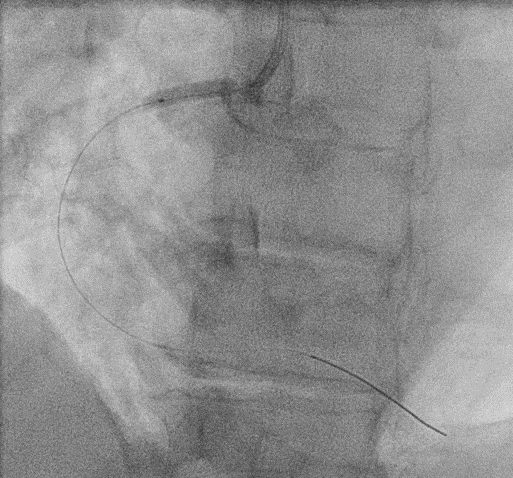
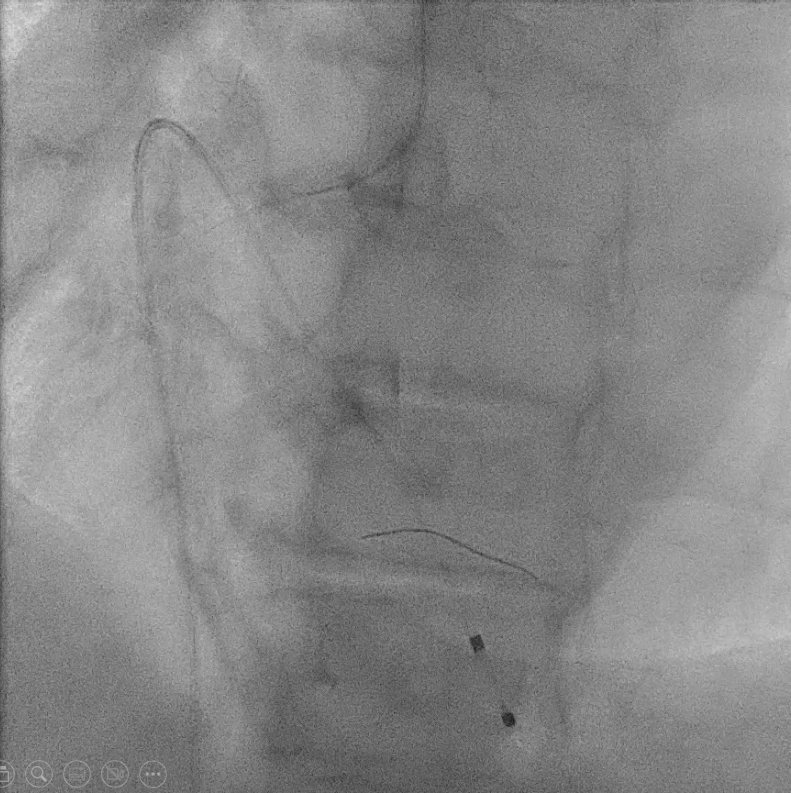
We first intervened the RCA. JR 4.0 6F was used as guiding catheter without fully engaging the RCA. Runthrough NS was threaded through ostial RCA by fishing technique and placed in PLV. Raiden 3.5/20 was used to predilate the ostial lesion with poor expansion. IVUS showed severe ostial RCA with circumferential calcification. We then proceeded to orbital atherectomy by exchanging to ViperWire and inserting temporary pacing lead. A total of 11 attempts of orbital atherectomy was performed (low speed x 7, high speed x4). Repeated inflation with Raiden 3.5/20 still had underexpansion at ostium. We then opted to perform intravascular lithotripsy with Shockwave 3.5/12 balloon. A total of 80 shocks was performed, after which good expansion of balloon was achieved. Xience 4.0/33 was deployed at ostial to proximal RCA at 12 atm. The stent was further optimized with NC Sapphire 4.0/15 at 14-22 atm and Accuforce 4.5/12 at 8-14 atm under IVUS guidance. Final angiogram showed satisfactory angiographic result with TIMI III flow and no dissection.
LAD intervention was relatively straightforward. Three drug-eluting stents were deployed after preparation with balloon angioplasty. Final angiogram showed satisfactory result.
LAD intervention was relatively straightforward. Three drug-eluting stents were deployed after preparation with balloon angioplasty. Final angiogram showed satisfactory result.
Case Summary
During intervention of severely calcified ostial lesion, conventional balloon angioplasty might be inadequate in the preparation of lesion for stenting. Orbital atherectomy could ablate the calcium with both forward and backward motion of the crown. If satisfactory expansion is still not achieved, this could be followed by intravascular lithotripsy to further crack the calcium ring. Before stenting, the expandability of the lesion should be confirmed with non-compliant balloon angioplasty. Moreover, intravascular imaging is essential in the assessment of coronary calcium, planning of procedure and evaluation of stent results.