
Lots of interesting abstracts and cases were submitted for TCTAP 2023. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-081
Now You Don't See It, Now You Do: Are We Missing the LAD?
By Chan Ho Thum
Presenter
Chan Ho Thum
Authors
Chan Ho Thum1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-081
CORONARY - Chronic Total Occlusion
Now You Don't See It, Now You Do: Are We Missing the LAD?
Chan Ho Thum1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
FBA
Relevant Clinical History and Physical Exam
44 year old diabetic hypertensive male smoker who was referred to us 4 months after developing anterior myocardial infarction, successfully thrombolyzed from a district hospital. He is currently asymptomatic with stable vital signs and physical examination was unremarkable
Relevant Test Results Prior to Catheterization
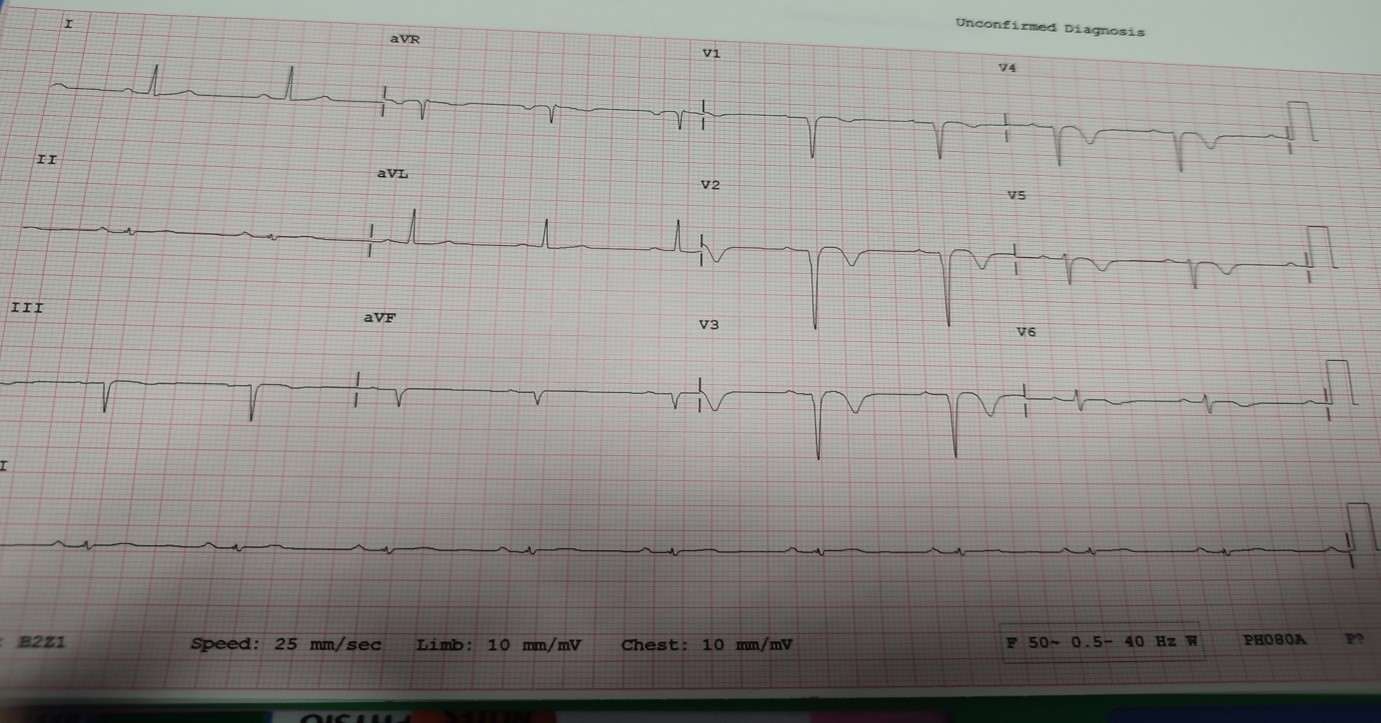
His ECG revealed Deep Q waves at the anterior leads with T Inversion at the anterolateral leads. Echocardiogram revealed an EF of 30% with hypokinesia predominantly at the LAD territory
 tctap 2023 echo.mpg
tctap 2023 echo.mpg
Relevant Catheterization Findings
Normal Left Main, Left Circumflex and RCA. Large Diagonal with many collaterals that can be mistaken for the LAD especially in the caudal and spider view. No obvious stump or retrograde flow that would indicate a CTO of the LAD. If we concentrate hard in the cranial view, there can be seen a very faint flow from the collaterals to the LAD region
Interventional Management
Procedural Step
We utilized an EBU 3.5, 6Fr guiding catheter with a Fielder XT wire. We crossed the suspected lesion partially but the wire kept buckling under pressure despite multiple attempts. We were unsure if it was in the true LAD lumen due to absence of retrograde flow to guide us. We reattempted with a Fine Cross Support. The Fielder wire was able to cross the initial resistance area smoothly. It was however, only directed medially and does not follow an LAD path. To avoid any potential complication, we switched the Fielder to a RTF wire. We gently predilated the area of suspected occlusion with Semi Compliant balloon 1.5/12 and noted slow flow down the vessel which appeared small. Further predilation with Semi Compliant balloon 2.0/15 revealed a significant LAD vessel. We rewired into the LAD and scored the distal to mid with a 2.0/15 Scoring balloon, followed by 2.5/15 Scoring Balloon at the mid LAD. We decided for a hybrid approach for the diseased LAD. After protecting the large D1 with an SB wire, we proceeded to deploy the Drug Coated Balloon from the mid to distal LAD. Due to dissection at the mid LAD, we stented the mid LAD overlapping the Drug Coated Balloon site distally with a 2.75/40 Drug Eluting Stent and postdilated it with Non Compliant Balloon 3.0/15 at high pressure proximally. The final results was acceptable with TIMI 3 flow.
Case Summary
It is important for us to treat all history of myocardial infarction with a high index of suspicion for probable occlusion of coronary vessels to avoid missing them. From this case, we also experience the challenge of attempting a recent CTO without a retrograde flow to guide us. Proper wires, support and technique is important for the success of the procedure. In addition, a hybrid combination approach with a Drug Eluting Stent proximally overlapping with a Drug Coated Balloon distally is an effective way to manage diseased long segments especially if it involves the distal vessels.