
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-038
Presenter
Tung-Lin Tsui
Authors
Tung-Lin Tsui1, Tung-Lin Tsui2, Chen-Yen Chien3
Affiliation
Camillian Saint Mary's Hospital Luodong, Taiwan1, Camillians Saint Mary's Hospital Luodong, Taiwan2, Mackay Memorial Hospital, Taiwan3,
View Study Report
TCTAP C-038
CORONARY - Cardiac Surgery/Hybrid Revascularization
Multiple Complication After Delayed Treated STEMI in COVID-19 Threatening
Tung-Lin Tsui1, Tung-Lin Tsui2, Chen-Yen Chien3
Camillian Saint Mary's Hospital Luodong, Taiwan1, Camillians Saint Mary's Hospital Luodong, Taiwan2, Mackay Memorial Hospital, Taiwan3,
Clinical Information
Patient initials or Identifier Number
817189
Relevant Clinical History and Physical Exam
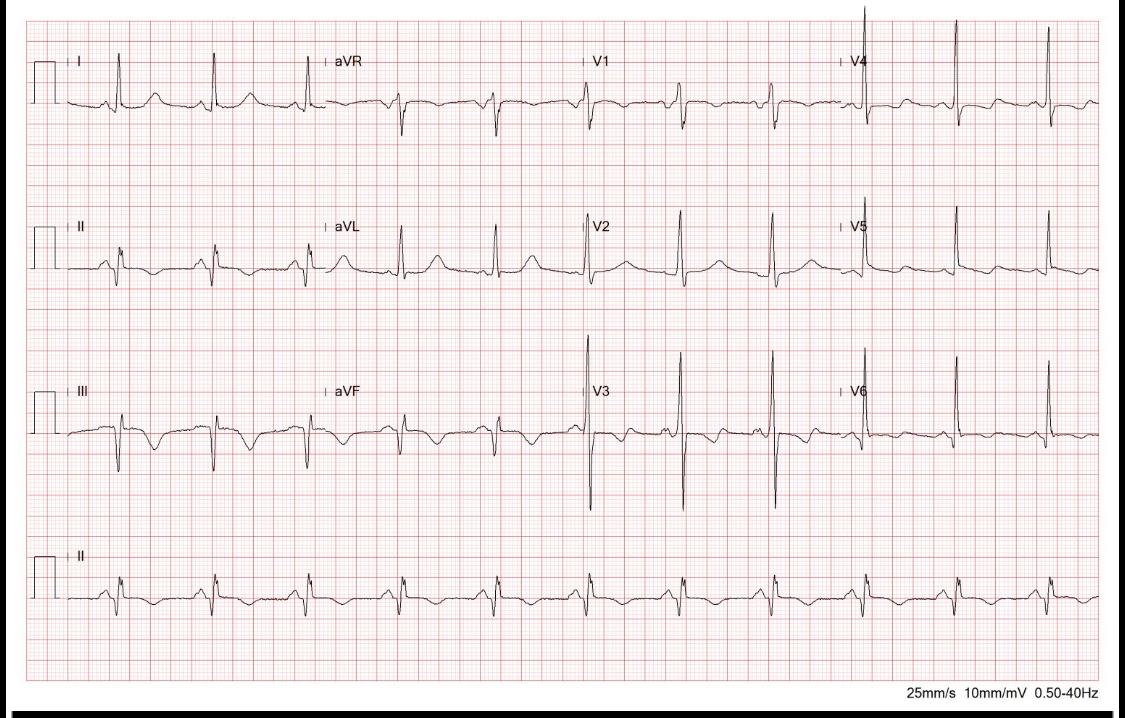
This is a 56-year-old gentleman who experienced severe chest tightness with cold sweating and mild fever since the morning. And he visited a local hospital for help. The initial EKG showed inferior lead ST elevation and ST depression over precordial leads. For further treatment, he was transferred to a regional hospital for primary PCI. CXR showed severe left lung infiltration.
Relevant Test Results Prior to Catheterization
However, due to the contact history of foreigners come from China and Japan, he was admitted to an isolation room and primary PCI was held. Instead of primary PCI, systemic urokinase infusion was arranged with 1500000u/day. The result of COVID-19 test showed negative 72 hours later, and the CXR showed no improvement. Leukocytosis with elevated CRP level was found, with acute kidney injury status.
Relevant Catheterization Findings
CAG was done and which showed a large thrombus over middle to distal RCA with TIMI 1-2 flow and critical stenosis over middle to distal LCX.
Interventional Management
Procedural Step
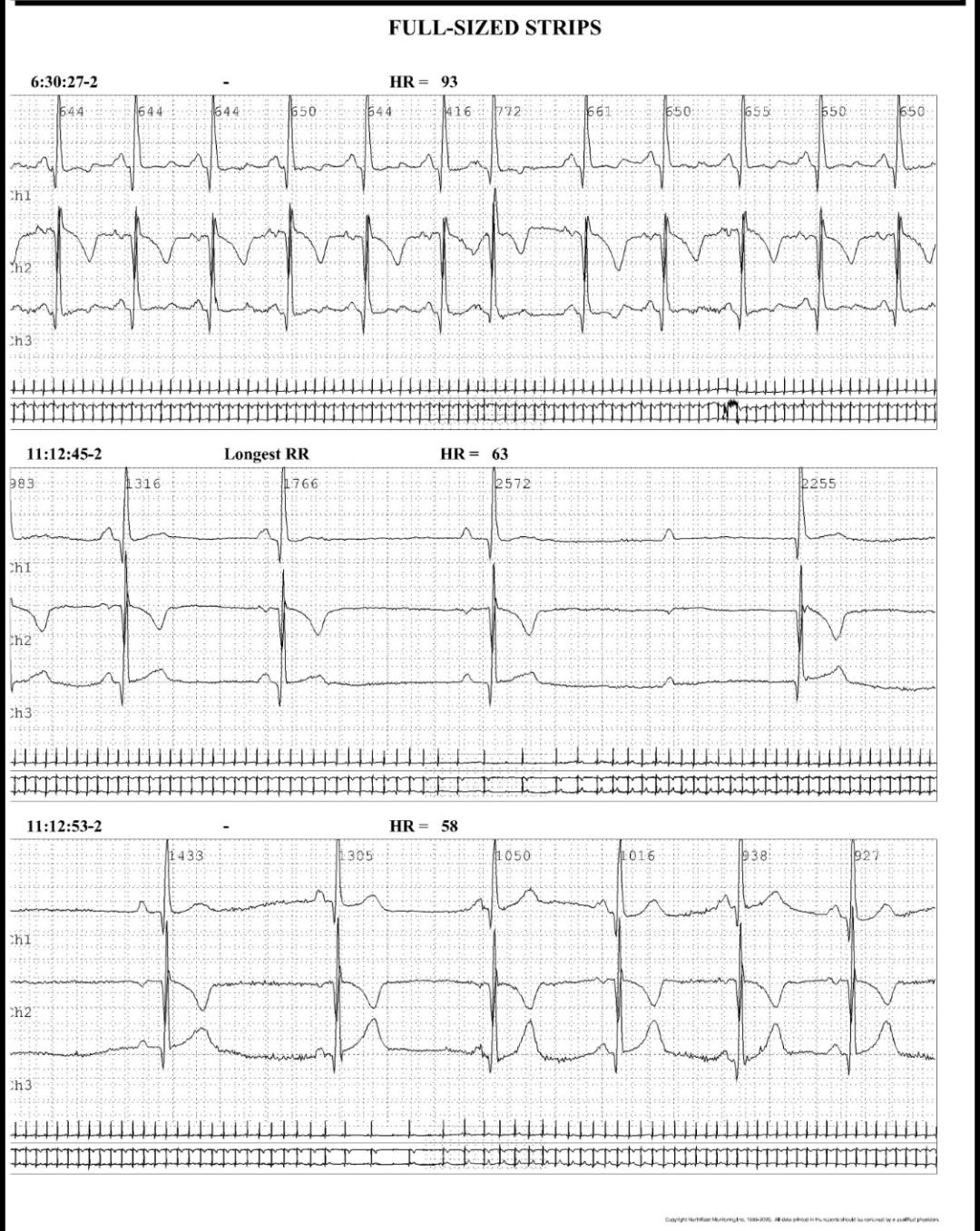
1. We wired a Floppy wire to distal RCA and thrombus suction was done 2..Some debris was aspirated out, without organized thrombus3. Balloon dilatation was done with Tazuna 3.0x20 balloon with 12 bars over distal RCA and 14 bars over middle RCA4. Residual stenosis over middle RCA was 65%5. Balloon dilatation was done with Ryurei 3.5x15 balloon with 14 bars over middle RCA 6. Residual stenosis over middle RCA was 40%7. A stent deployment was done, with Merit Biomime 3.5x32 drug-eluting stent.8. Post dilatation with 3.5x15 NC balloon with 16 bars and final result was good, TIMI 3 flow.9. Chest tightness and cold sweating improved very much. But recurrent angina was noted 4 days later, with new T wave inversion over inferior leads and V5-V610. Second look CAG showed good RCA flow but poor LCX flow.11. PCI for LCX middle to distal critical lesion was done with Tazuna 2.5x20 balloon12. Dissection was noted with residual stenosis over middle to distal LCX was 50%13. A stent deployment was done, with Elixir Desyne 2.5x28 drug-eluting stent.14. Final result was good, TIMI LCX flow.15. Intermittent bradycardia and AV block were noted, long pause and near syncope were found.16. Pacemaker implantation was done for second degree AV block17. Refractory pulmonary edema and pleural effusion was noted and follow up heart echo showed severe MR.18. Surgical intervention with mitral valve replacement was done.19. No more pulmonary edema and pleural effusion20. OPD follow up 6 months already.
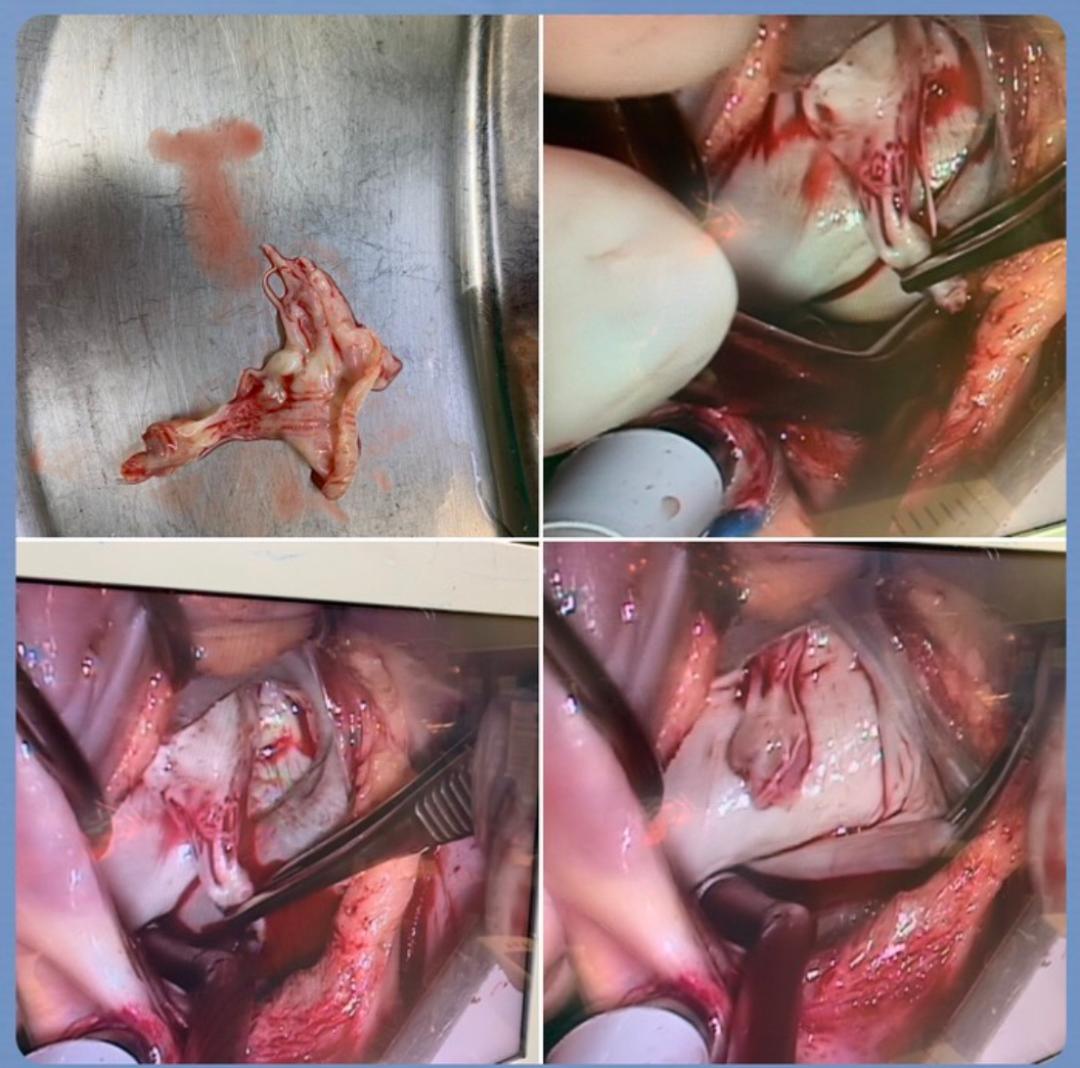
Case Summary
The most suggested management for STEMI was primary coronary intervention, besides, after successful revascularization for culprit lesion, if critical stenosis which may have potency to become acute infarction, we can do coronary intervention for the lesion as the same operation. However, because of the threatening of COVID-19, some primary coronary intervention may be held, which may induce more myocardial damage, and cause conduction system defect or delayed papillary muscle rupture. We suggested that if conduction system defect was noted, repeated echocardiography was necessary for heart structure and function study.