
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-109
Presenter
Keshavamurthy Ganapathy Bhat
Authors
Davinder Singh Chadha1, Keshavamurthy G2
Affiliation
Manipal Hospital, India1, Ahrr, India2,
View Study Report
TCTAP C-109
STRUCTURAL HEART DISEASE - Others (Structural Heart Disease)
Post Myocardial Infarction Ventricular Septal Rupture with Heart Failure Treated Successfully with Transcatheter Device Closure
Davinder Singh Chadha1, Keshavamurthy G2
Manipal Hospital, India1, Ahrr, India2,
Clinical Information
Patient initials or Identifier Number
VDVL
Relevant Clinical History and Physical Exam
A 69-year-old gentleman, tobacco chewer, presented with anginal chest pain of 8 hours duration. Clinically he had tachycardia. Other vitals and systems- unremarkable. ECG showed ST elevation in leads II, III and AVF. 2D Echocardiography showed RWMA in inferior wall with LVEF 55%. He was immediately taken up for Primary Angioplasty.

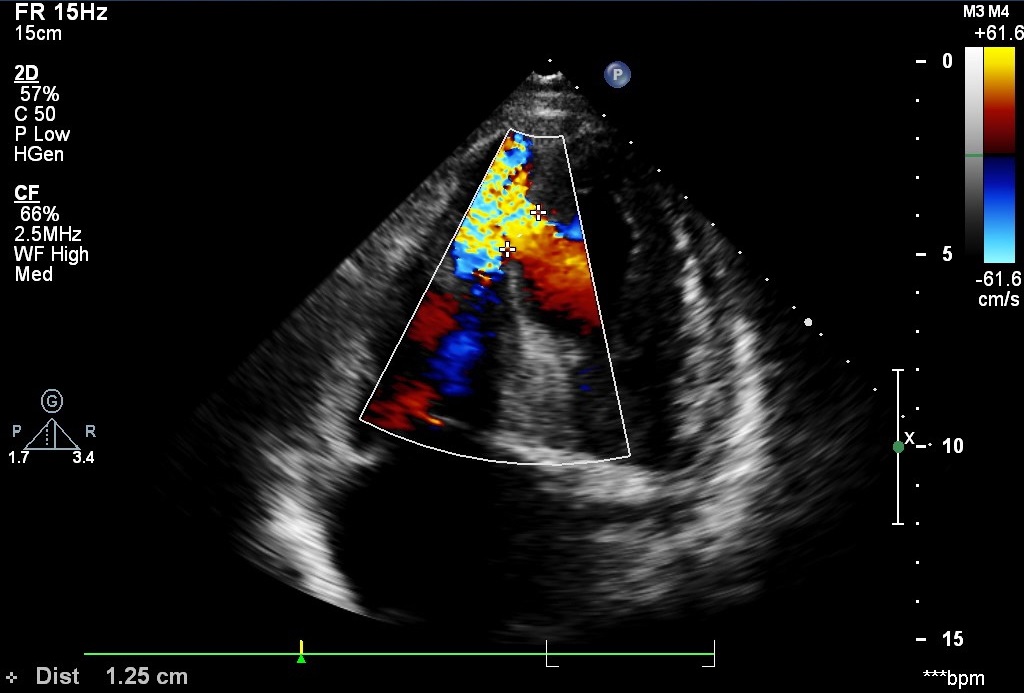
Relevant Test Results Prior to Catheterization
Echocardiography showed 14 mm Ventricular Septal Rupture in apical inferior septum with left to right shunt. PA pressure was 60 mmHg.
 POST MI VSD F_O NC VADIVEL20180920174551997 (Converted).mov
POST MI VSD F_O NC VADIVEL20180920174551997 (Converted).mov
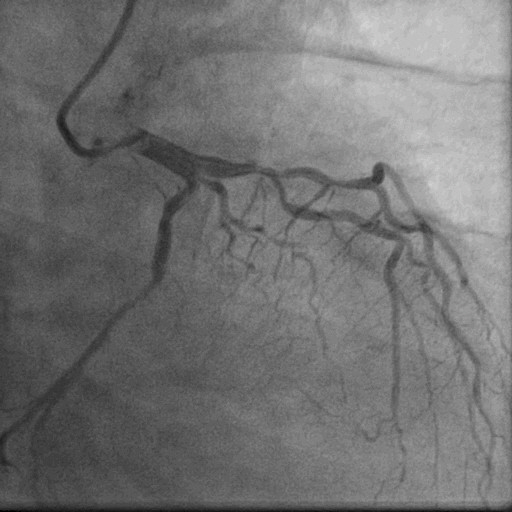
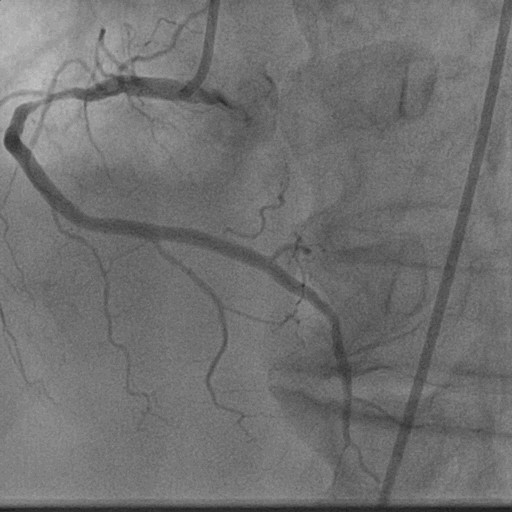
Relevant Catheterization Findings
After 3 weeks of anti-failure therapy, he was taken up for percutaneous device closure of Ventricular Septal Rupture (VSR).
LV Angio (Converted).mov

Interventional Management
Procedural Step
The procedure was meticulously planned including access, hardware, possible complications, and solutions. Surgical team was kept stand by. It was decided to establish arteriovenous loop from right femoral artery to right internal jugular vein (RIJV) so that it becomes easier to negotiate apical VSR while bringing delivery sheath from RIJV.Accesses were: Right Femoral Artery (RFA) -6F, Right Femoral Vein (RFV)- 6F. Right internal jugular vein (RIJV) – 6F. VSD crossed with exchange length 0.035” Terumo glide wire taken in a JR 6F guiding catheter. Terumo wire negotiated into PA. It was snared from Rt IJV through a gooseneck snare and exteriorized. Thus AV Loop established. Thereafter 18 mm Amplatzer Muscular VSD device was loaded onto a 9F loader. 9F delivery sheath taken over Terumo wire into LV. Terumo removed. Device loaded into delivery sheath and taken to LV. LV disc deployed in LV. Device pulled back into VSD and RV disc deployed. Check angio showed minimal residual flow across. Echo also showed snuggly fitting device across VSR. Device released. Procedure completed without any complications.Three days later, Echo showed complete closure of VSR without any residual flow.
Device deployed in VSR (Converted).mov
Device released (Converted).mov
Echo post closure Follow up VSR (Converted).mov
Case Summary
Ventricular Septal Rupture(VSR) is a rare but life-threatening complication of Acute Myocardial Infarction. Wherever feasible, complete revascularisation and stabilization should be done before attempting closure of VSR to allow the margins of VSR to heal and become firm. In this patient, we performed multivessel PCI(TVD) and stabilized heart failure before device closure. One needs to oversize the device by at least 4-6 mm unlike congenital VSD. Ideally, post MI VSR device to be used which has a wider LV disc and longer waist.