
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-063
Presenter
Mohammad Shafiqur Rahman Patwary
Authors
Mohammad Shafiqur Rahman Patwary1
Affiliation
Kurmitola General Hospital and Armed Forces Medical College, Bangladesh1,
View Study Report
TCTAP C-063
CORONARY - Complications
Is Exaggeration of Non-culprit Stenosis Following PCI?
Mohammad Shafiqur Rahman Patwary1
Kurmitola General Hospital and Armed Forces Medical College, Bangladesh1,
Clinical Information
Patient initials or Identifier Number
ID- 6781-0
Relevant Clinical History and Physical Exam
Mr. X, 65 years old gentleman, normotensive, non-diabetic, smoker presented with complaints of central chest pain radiate to left arm.


On examination, pulse was 80/minutes. Blood pressure was 130/80 mmHg. S1 and S2 were normal. Lung base was clear.
He also developed sudden cardiac arrest in hospital and was managed with prompt emergency treatment.
He gave a history of PCI to LCX and OM1 one month back.
He was labelled as NSTEMI with post PCI status and managed conservatively with LMWH.
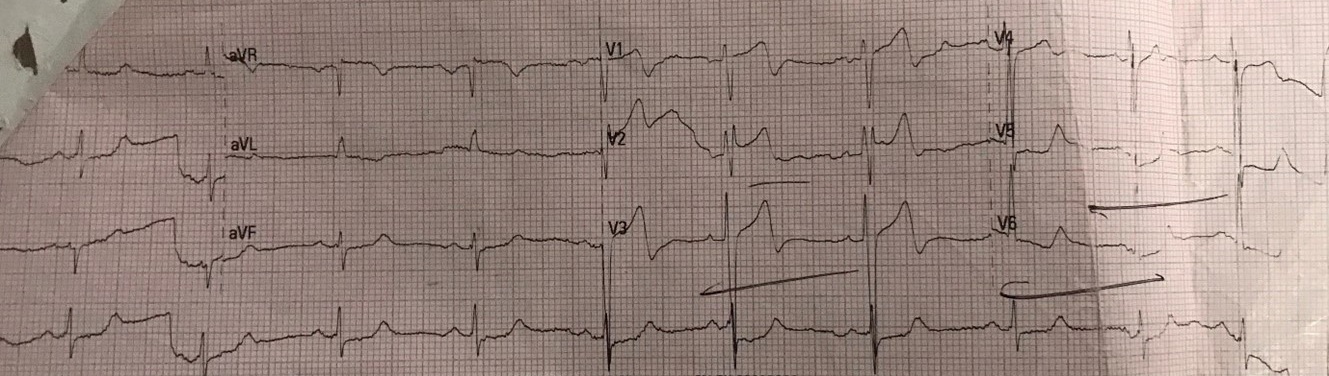
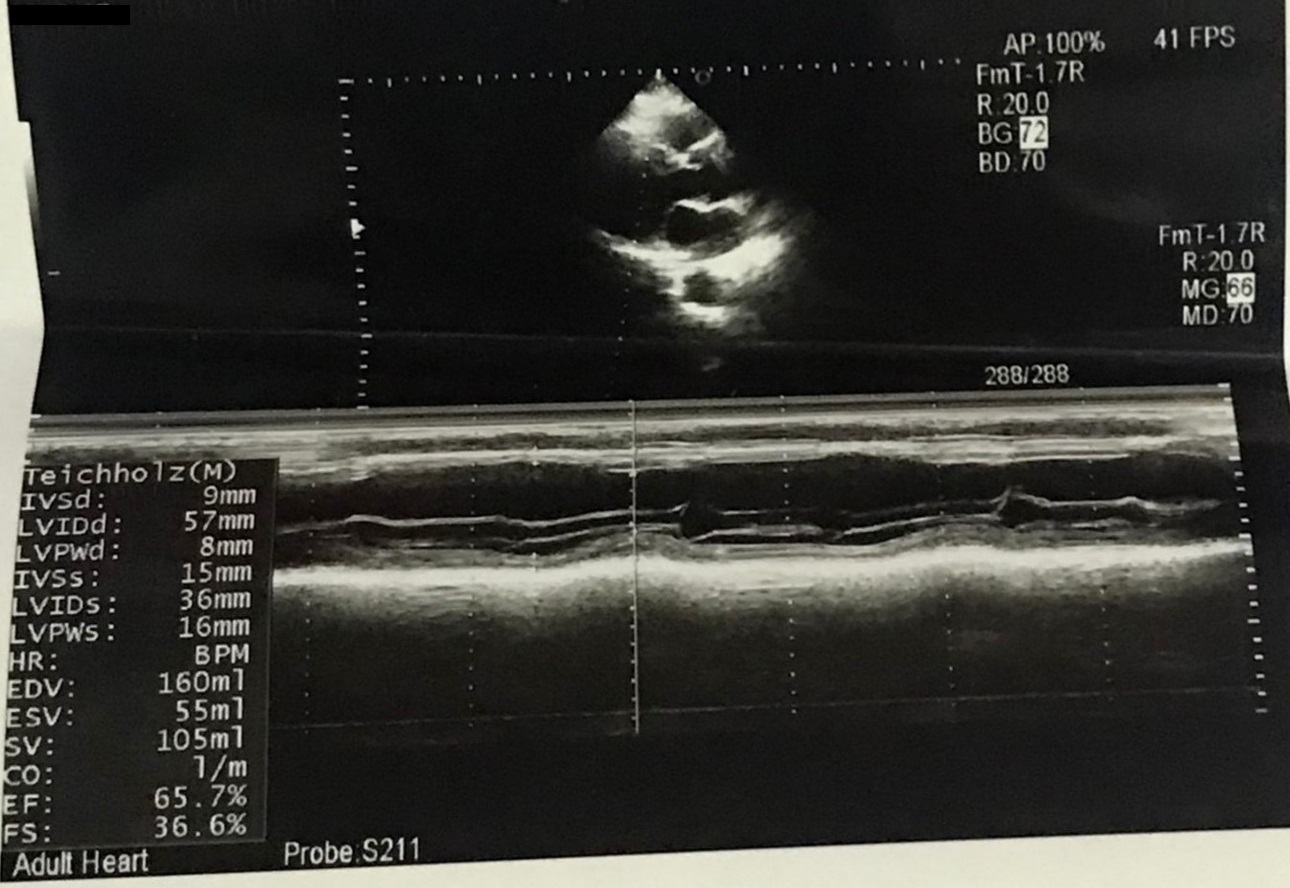
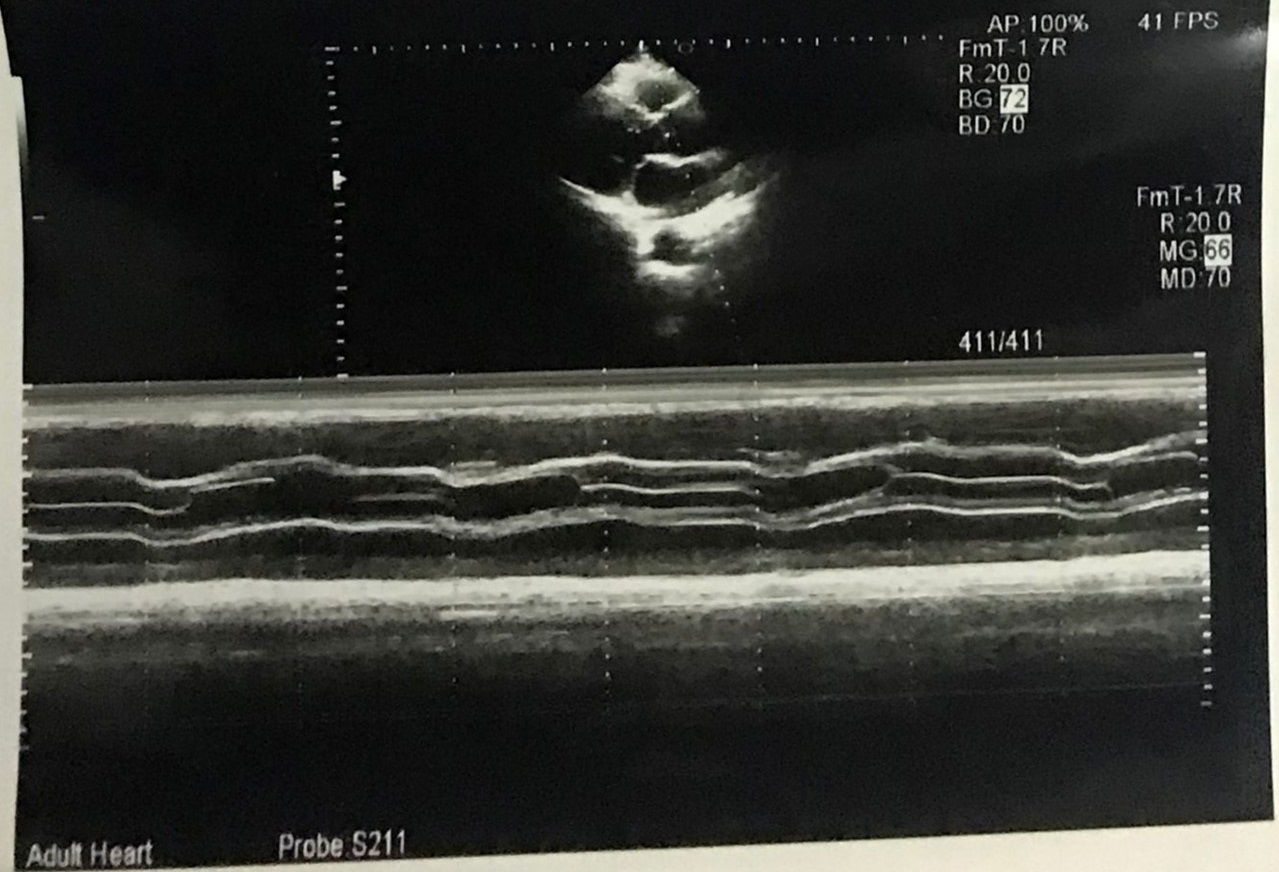
Relevant Test Results Prior to Catheterization
Electrocardiogram showed anterior ischaemic changes.Echocardiogram showed anterior wall hypokinetic with LVEF 65 %.Serum Troponin Iwas 8.0 ng/Ml.HbA1c was5.6%.
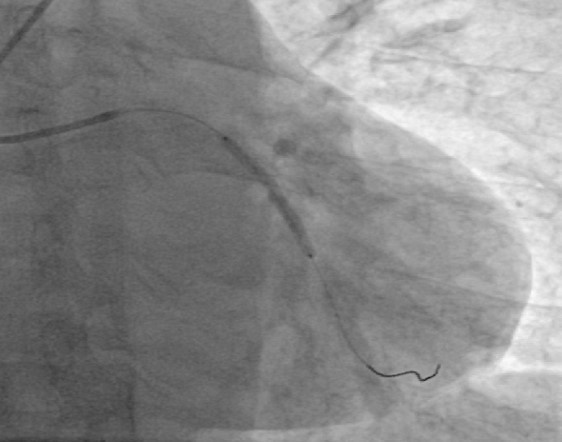
Relevant Catheterization Findings
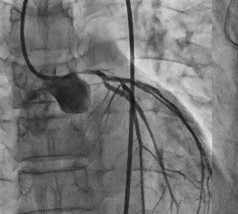
Check CAG through RFA revealsLeft Main: 95% stenosis in osteoproximal. LAD: Minor plaque in proximal part, type III vessel.LCX: Patent stent in mid LCX and OM1, dominant vessel. RCA: Normal and non dominant. Diagnosis: LM involvement with patent stent in LCX and OM1 Suggestion: PCI to left main.

Interventional Management
Procedural Step
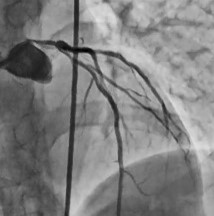
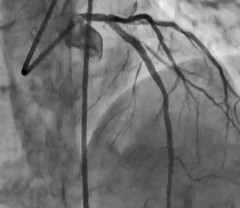
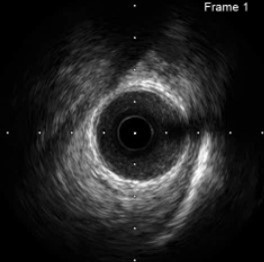
EBU 3.5 ,6F guide catheter was used. Rinato and All star wires were crossed the lesion and parked in the distal part of the LAD and LCX respectively. Pre dilatation was done by Maverick 2.5 mm X 15mm semi complaint balloon at 14 atm. IVUS images were taken before stenting. Synergy 3mm X 48 mm stent was deployed in the left main covering the proximal part of LAD at 16 atm. Post dilatation was done with NC Quantum 4mm X 12mm balloon at16 atm. After post dilatation, IVUS study was repeated. Procedure was uneventful.

Case Summary
Our patients had PCI to OM1 and LCX one month ago for unstable coronary disease. He was well and uneventful. After one month of PCI, admitted with cardiac arrest and Non STEMI. He had no or minimal lesion in osteo proximal part of the LM previously when he underwent PCI. Now his both stent had no stenosis with TIMI flow III, but LM had critical stenosis. We manage it with stenting to LM and proximal LAD with IVUS imaging. Is first PCI can induce lesion in LM?