
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-064
Presenter
Sirichai Wiriyatanakorn
Authors
Sirichai Wiriyatanakorn1, Krissada Meemook1
Affiliation
Ramathibodi Hospital, Thailand1,
View Study Report
TCTAP C-064
CORONARY - Complications
It Never Rains But It Pours
Sirichai Wiriyatanakorn1, Krissada Meemook1
Ramathibodi Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
TJ
Relevant Clinical History and Physical Exam
TJ is a 47 years old man with hypertension, hyperlipidemia, post-kidney transplantation, and ex-smoker. He presented to rural hospital 2 months ago with myocardial infarction and received medical treatment with antiplatelets and low-molecular-weight heparin until discharge. He was in NYHA functional class II. After that, He visited Ramathibodi Hospital and was scheduled for elective coronary angiography this time. His physical examination was unremarkable.
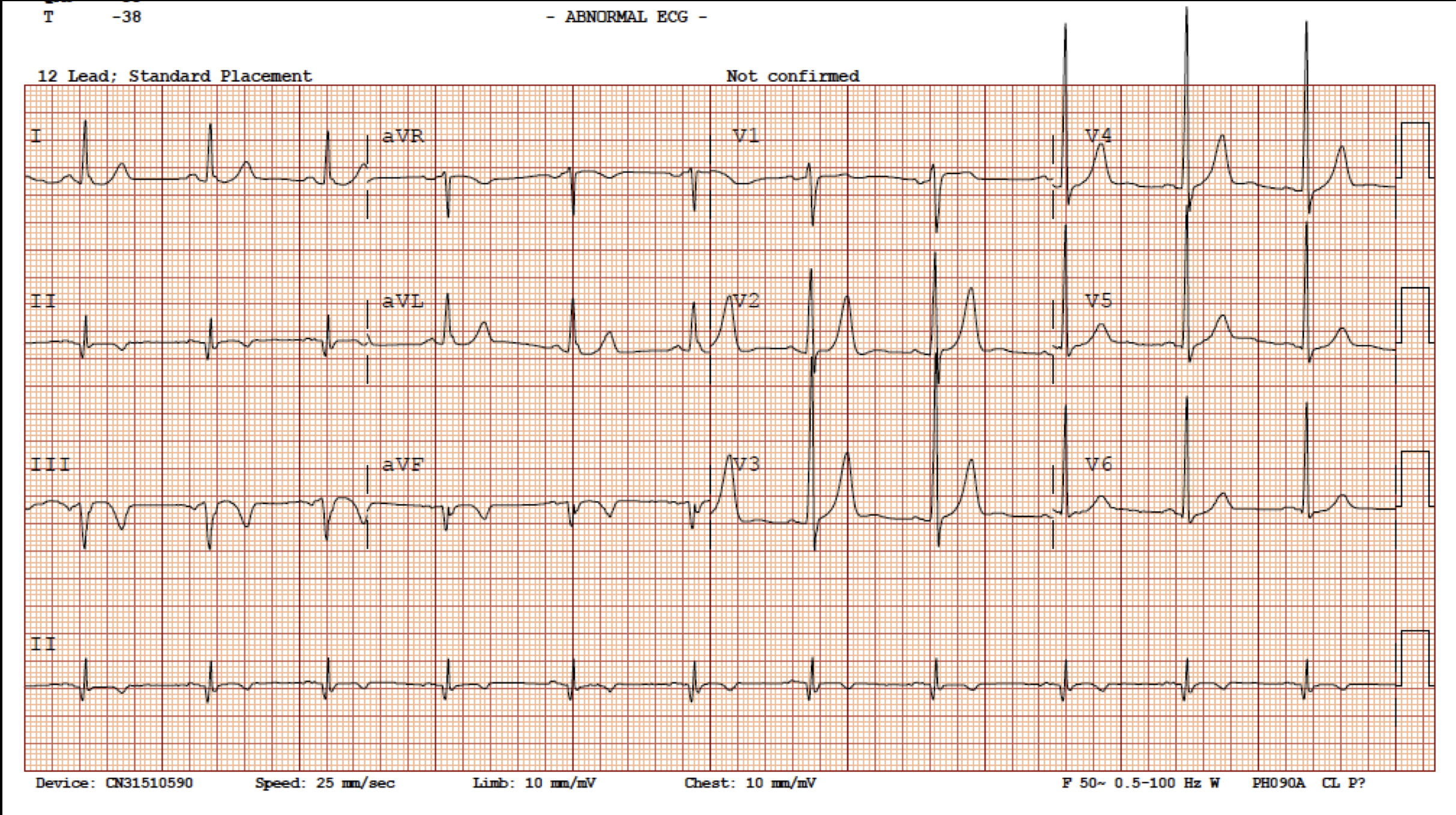
Relevant Test Results Prior to Catheterization
His ECG showed sinus rhythm rate 66 bpm with Q wave and T wave inversion at II, III, and aVF leads. His chest X-ray was unremarkable. Echocardiogram showed LV ejection fraction about 50-55% and hypokinesis at inferior wall with preserved LV thickness.

Relevant Catheterization Findings
We performed coronary angiogram via right radial approach using 5F JR 3.5 and JL 3.5 diagnostic catheters. The angiogram of right coronary system showed diffuse severe stenosis of RCA with TIMI 2 flow. The angiogram of left coronary system showed focal moderate to severe stenosis of mid LAD, distal LAD, and diagonal branch, as well as moderate to severe stenosis of proximal LCx.
 RCA CINE.mov
RCA CINE.mov
Left CINE.mov
Interventional Management
Procedural Step
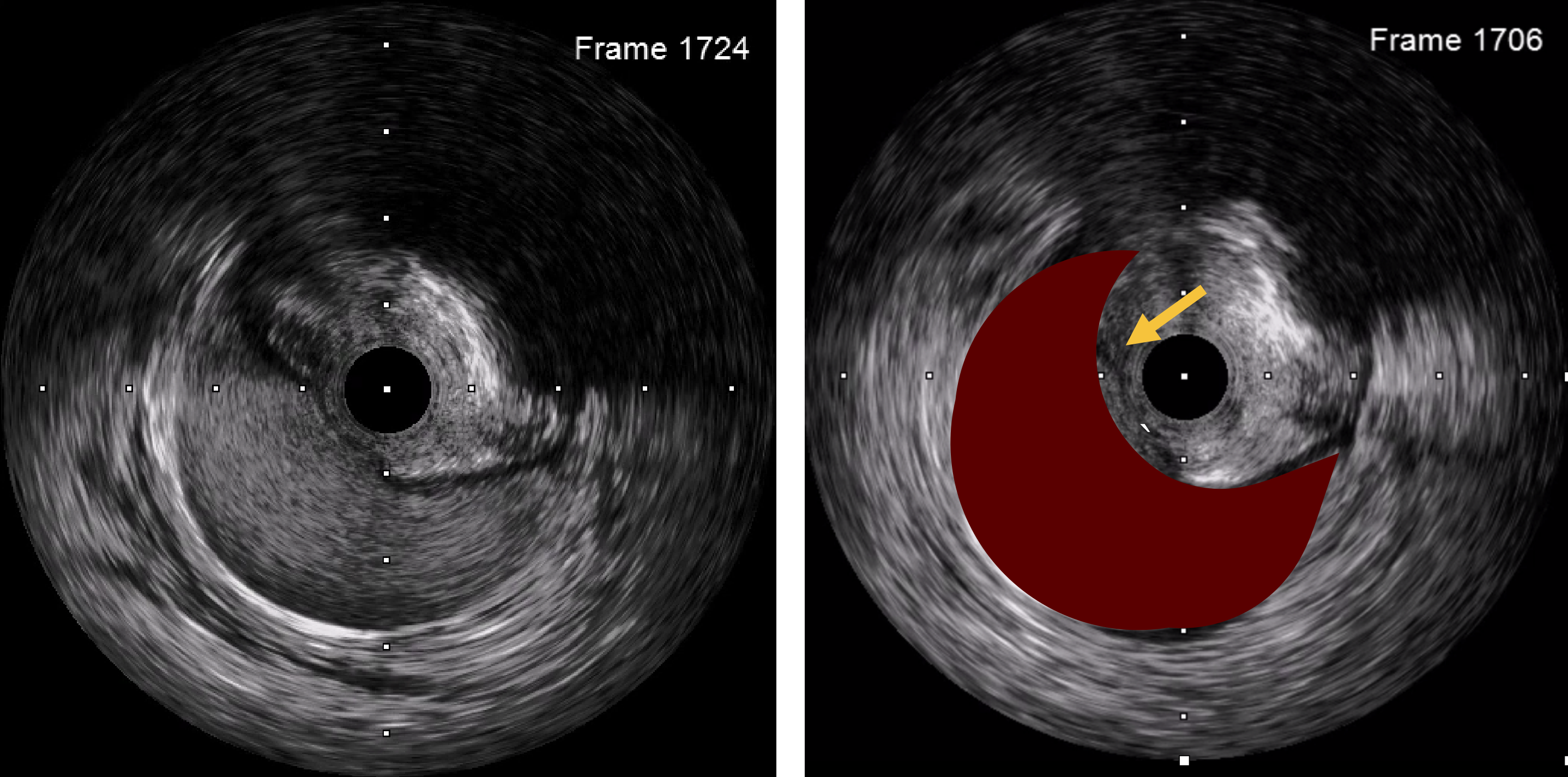
In this case, we had discussed the choice of revascularization to the patient and his relatives. We, and the patient, decided to do multivessel PCI for complete revascularization. We planned to perform PCI to RCA in this visit and scheduled for stage PCI in the future.We used 6F guiding AL1 short tip catheter and Asahi Fielder FC guidewire passing through the distal RCA. We then dilated the lesions with semi-compliance balloon size 1.5 and 2.5 mm, respectively. After pre-dilation at the proximal segment, there was some contrast staining located distal to guiding catheter. Suddenly, someone injected the dye without recognition. What happened next was extensive RCA dissection. Unfortunately, when we tried to withdraw the catheter, everything including guidewire totally lost from the vessel.We attempted to recross the wire to RCA without contrast injection to minimize the risk of dissection progression. We used very soft wire (Runthrough NS) and multiple orthogonal views to help re-crossing the wire. After re-crossing, we used IVUS to confirm that wire was in true lumen. IVUS also showed that there was dissection and large hematoma of RCA. Subsequently, we decided to stent the proximal segment first to seal and reduce further dissection. We used 4.0 mm DES for proximal segment. Then, we stented the rest of RCA from distal to mid portion with 2.5, 3.0, and 3.5 mm DES, respectively. Then, we used the IVUS to guide post-dilation. Final angiogram and IVUS showed good result and TIMI 3.
Extensive RCA dissection.mov
Final angiogram.mov
Case Summary
A case with extensive RCA dissection from catheter-induced injury and forceful contrast injection and accidentally wire lost after dissection. Re-crossing wire was done with soft tip guidewire and adjunct IVUS imaging, then successfully treated all the lesions.
Learning Points:- Careful guiding catheter manipulation is mandatory.- Securing and maintaining wire access across the dissected artery is the most important.- Use soft-tip wire and multiple views for rewiring. Avoid contrast injection to minimize risk of further injury.- Intravascular imaging is very helpful for treatment of the complication.- Seal the proximal dissection first to reduce dissection and hematoma progression.
Learning Points:- Careful guiding catheter manipulation is mandatory.- Securing and maintaining wire access across the dissected artery is the most important.- Use soft-tip wire and multiple views for rewiring. Avoid contrast injection to minimize risk of further injury.- Intravascular imaging is very helpful for treatment of the complication.- Seal the proximal dissection first to reduce dissection and hematoma progression.