
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-094
Presenter
Chen Ting Tan
Authors
Chen Ting Tan1, Alan Fong1
Affiliation
Sarawak Heart Centre, Malaysia1,
View Study Report
TCTAP C-094
IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular
"SAME" ACS
Chen Ting Tan1, Alan Fong1
Sarawak Heart Centre, Malaysia1,
Clinical Information
Patient initials or Identifier Number
AK
Relevant Clinical History and Physical Exam
A 43-year-old gentleman, an ex-smoker with underlying double vessel disease and history of PCI to RCA with 2 drug eluting stents (DES) in September 2017. He presented with central chest pain for 4 hours prior to the hospital visit.

Relevant Test Results Prior to Catheterization
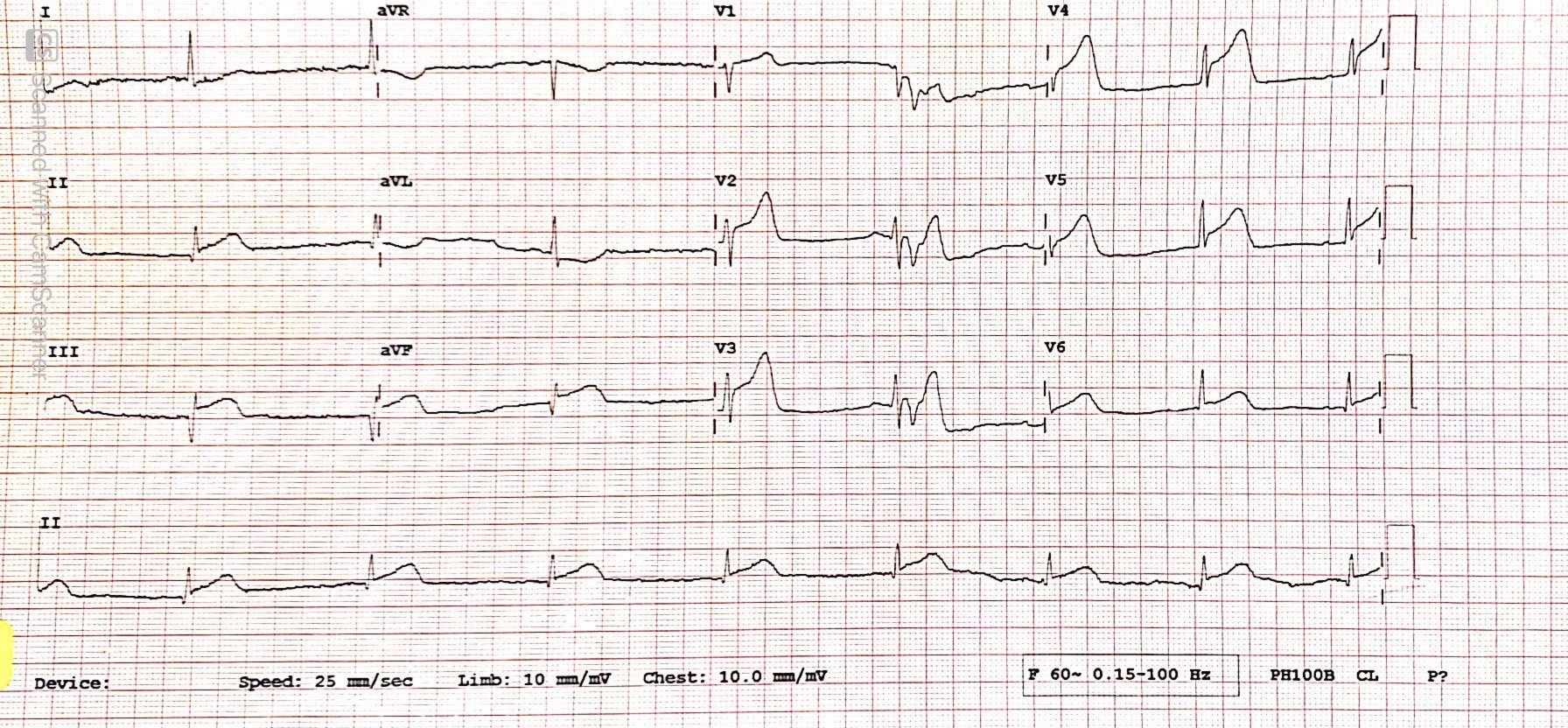
ECG showed extensive ST elevation in V2-V5, II, III, aVF. No posterior or right sided involvement. He was treated by thrombolysis (IV Metalyse 10,000U) but was unsuccessful. Therefore, he was treated with rescue PCI.
 ak 1(3).mp4
ak 1(3).mp4
ak 1(4).mp4
ak 1(5).mp4
Relevant Catheterization Findings
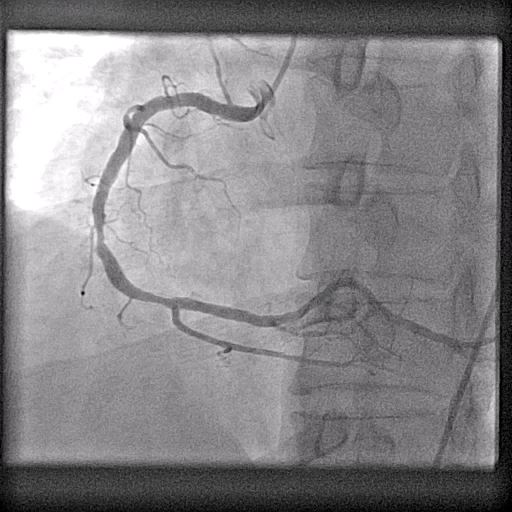
Coronary angiogram showed proximal LAD 90% stenosis and mid RCA 70% stenosis. LMS and LCX normal. Decided PCI to LAD.
ak 1(6).mp4
ak 1(9).mp4
ak 1(10).mp4
Interventional Management
Procedural Step
After the BMW guidewire crossed the lesion, angiography revealed the “lesion” was a thrombus and it migrated to distal LAD. OCT confirmed plaque rupture with minimum lumen area (MLA) of 4.97mm2. In view of adequate lumen area and angiography TIMI III flow, we decided to leave the lesion without stenting. Thrombo-aspiration over the distal LAD, yielded some thrombus. IV Tirofiban infusion was commenced for 24 hours. Subsequent Echocardiogram showed LVEF 35.2% with RWMA. After completed ACS treatment for 3 days, he was discharged with aspirin and clopidogrel. A re-look angiogram was done at 1 month showed proximal LAD 30% stenosis and OCT confirmed healed plaque ruptured with MLA of 5.38mm2. Clinically, he was well no angina, NYHA Class 1 and had no heart failure symptoms.
oct_3 Nov 2020 10-44-17.mp4
oct.mp4
ak 2(2).mp4
Case Summary
ACS is a leading cause of death worldwide and plaque rupture accounted for nearly two-third of cases. Optical coherence tomography (OCT) enables us to identify the mechanism of ACS, thereby providing precise and personalized therapy. Erosion study has shown that OCT identified plaque erosion will be benefited from antithrombotic therapy alone without stent implantation. In our case, OCT showed plaque rupture with adequate lumen area had late lumen gain at 1 month without stenting. Therefore, not all the plaque rupture is the same and further study is needed to validate this.