
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-051
Presenter
Harinder K. Bali
Authors
Harinder K. Bali1, Amreen Dhindsa2, Navdeep Singh Sidhu3, Fazal Karim4, Surinder Bali5
Affiliation
Paras Hospitals, India1, Fortis Hospital, India2, AIIMS Bilaspur HP, India3, PGIMER, India4, Ex professor GMC Jammu, India5,
View Study Report
TCTAP C-051
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
Left Main Equivalent Bifurcation Stenting of Saphenous Venous Graft Lesion in a Patient with a Previous Rare Saphenous Venous Graft Intervention
Harinder K. Bali1, Amreen Dhindsa2, Navdeep Singh Sidhu3, Fazal Karim4, Surinder Bali5
Paras Hospitals, India1, Fortis Hospital, India2, AIIMS Bilaspur HP, India3, PGIMER, India4, Ex professor GMC Jammu, India5,
Clinical Information
Patient initials or Identifier Number
NL
Relevant Clinical History and Physical Exam
83 years old male, K/C/O Coronary artery diseasePresented with retrosternal chest discomfort & dyspnoea on exertion grade 2/3 worsening to grade 4.Relevant Past history:Underwent CABG in 2011 (SVG to LAD / obtuse marginal (jump graft), SVG to posterior left ventricular artery. Underwent stenting to left main to LAD (crossover) in 2013.Underwent angioplasty of ostial flush occlusion of SVG to LAD/ obtuse marginal jump graft via retrograde approach through native LCx in 2015 (first in the world)
Relevant Test Results Prior to Catheterization
2D echocardiography revealed preserved LV function with no regional wall motion abnormality.
Relevant Catheterization Findings
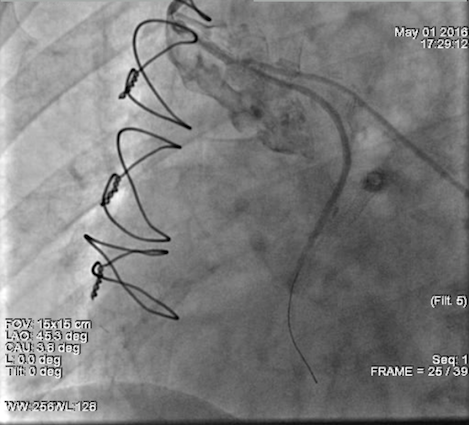
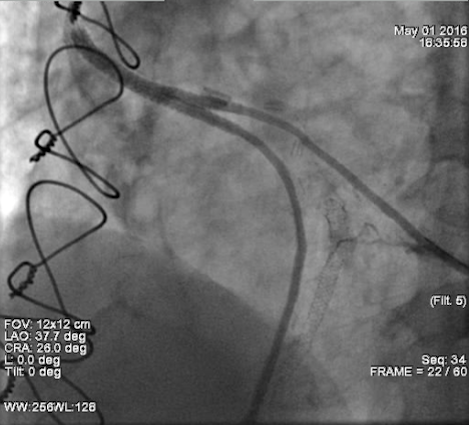
Native TVDPatent LM to LAD stent mid LAD- l00% stenosisLCX non-dominant, diffusely diseased small caliber vessel RCA dominant, diffusely diseased with 90-95% stenosisRSVG to PLV patent SVG to left anterior descending/ obtuse marginal jump graft proximal 90% in-stent restenosisSignificant medina 1,1,1 disease at SVG to left anterior descending/ obtuse marginal graft bifurcation
Interventional Management
Procedural Step
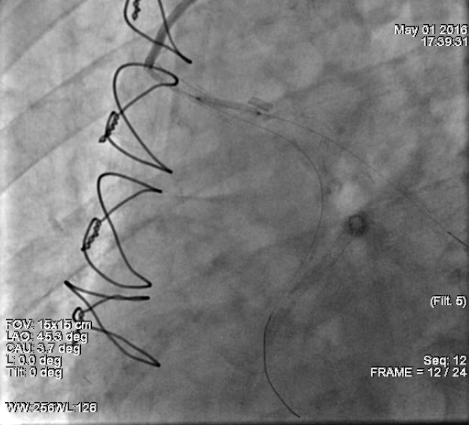
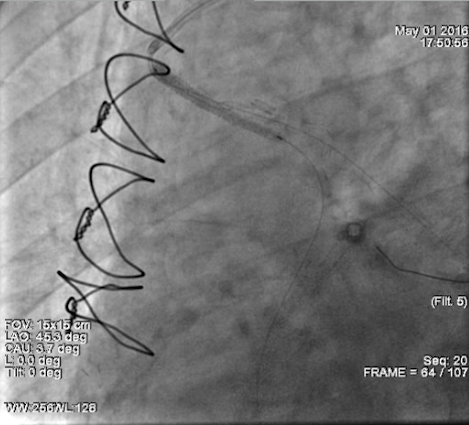
Mini crush techniqueRoute : right femoral artery Hardware: Guide catheter : 7F AR Guide Wire: BMW Stents: XIENCE XPEDITION stent 2.5 X 18 mm RSVG to OM; XIENCE XPEDITION LL stent 2.5 X 38 mm RSVG to LAD.Steps: 7F AR guide inserted, BMW wire introduced into the periphery of SVG to LAD (main branch), followed by balloon angioplasty of the proximal ISR of jump graft.Second BMW wire introduced into periphery of OM branch of the jump graft (side branch), Pre stent dilatation of main branch done.Pre stent dilatation of side branch done.Balloon catheter placed across the main branch, Xience Xpedition stent 2.5 mm x 18 mm, placed in the side branchStent deployed in side branch with its proximal part protruding slightly proximal to the carina of the bifurcation Balloon in main branch inflated, crushing the proximal edge of side branch stentXience Xpedition LL stent (2.5 X 38 mm) deployed in the main branch Post stent dilatation of main branch and side branch done followed by simultaneous kissing dilatation and proximal optimisationSatisfactory final outcome with TIMI 3 flow achieved
Case Summary
Bifurcation stenting of the RSVG-LAD/OM graft was done, which can be considered equivalent to a left main bifurcation intervention.This is one of the only few cases of successful RSVG bifurcation stenting reported worldwide. This case demonstrates that the mini crush technique is feasible for PCI in bifurcation lesions of the SVG and provides a satisfactory angiographic result and favorable clinical outcome.