
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-045
Presenter
Khin Maung Zan @ Mohd Saad Jalaluddin
Authors
Khin Maung Zan Mohd Saad Jalaluddin1
Affiliation
Hospital Pusrawi, Malaysia1,
View Study Report
TCTAP C-045
CORONARY - Chronic Total Occlusion
Percutaneous Coronary Intervention of Calcified CTO RCA in a Symptomatic Elderly Patient
Khin Maung Zan Mohd Saad Jalaluddin1
Hospital Pusrawi, Malaysia1,
Clinical Information
Patient initials or Identifier Number
THS
Relevant Clinical History and Physical Exam
80-year-old lady presented with central chest pain for 2 days associated with diaphoresis. She has underlying Type 2 Diabetes mellitus, Hypertension and Chronic kidney disease stage 3. Clinical examinations were generally unremarkable with blood pressure of 135/70 mmHg with heart rate of 72 beats per minute. Electrocardiogram showed T wave inversion at leads II, III and aVF. Her echocardiogram showed LVEF of 57% with regional wall motion abnormalities at inferior wall.
Relevant Test Results Prior to Catheterization
Baseline creatinine- 113
NT-proBNP- 87
hs Troponin T- 17HbA1C- 6.3LDL-C 1.3
Relevant Catheterization Findings
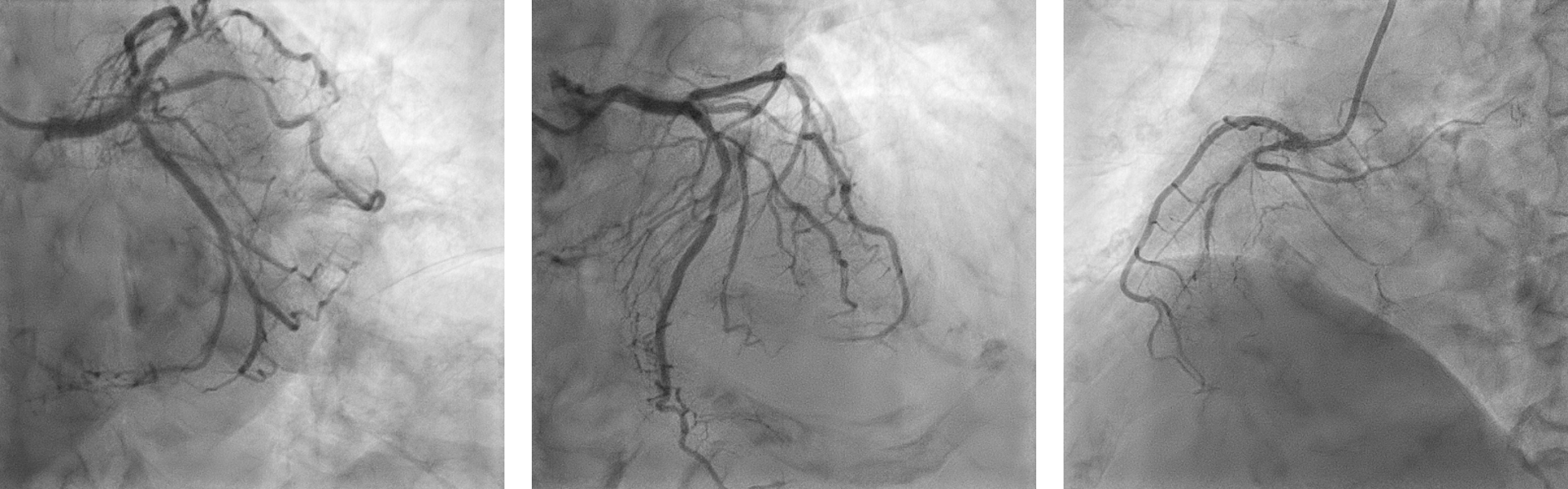
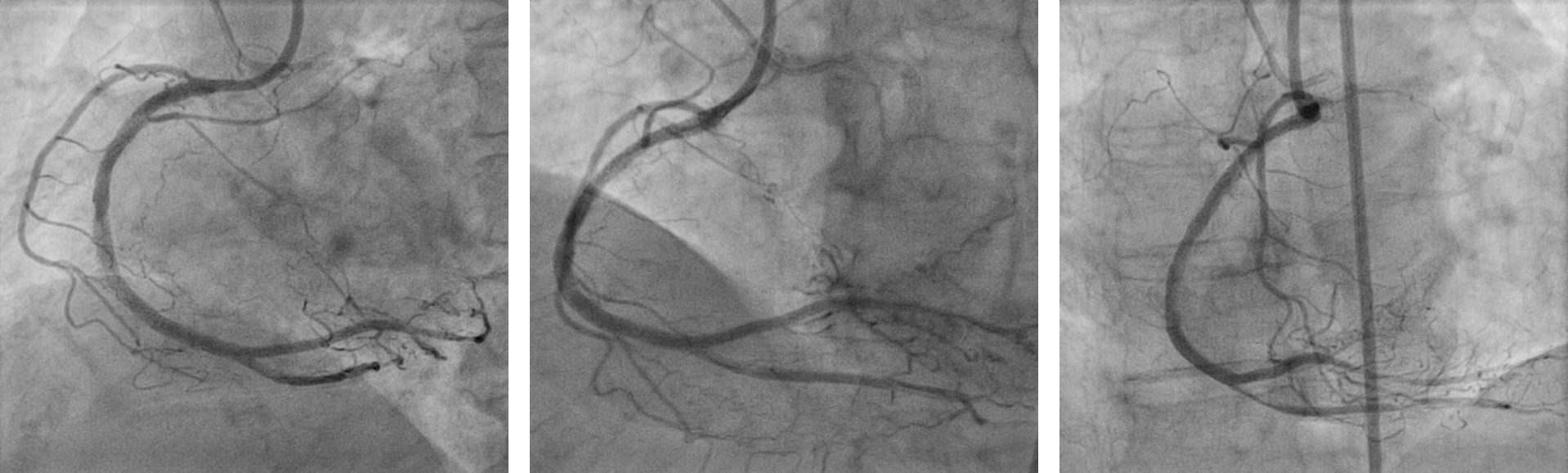
Coronary angiogram showed mild disease of left main stem and ostial left circumflex artery, severe stenosis of intermediate artery and mid left anterior descending artery, calcified and severe diffuse disease of proximal right coronary artery with chronic total occlusion from mid segment. There was retrograde flow to distal right coronary artery from left circumflex and left anterior descending arteries. In view of high Syntax I and Syntax II scores, she was offered CABG but not keen.
 CAG 1.avi
CAG 1.avi
CAG2.avi
CAG3.avi
Interventional Management
Procedural Step
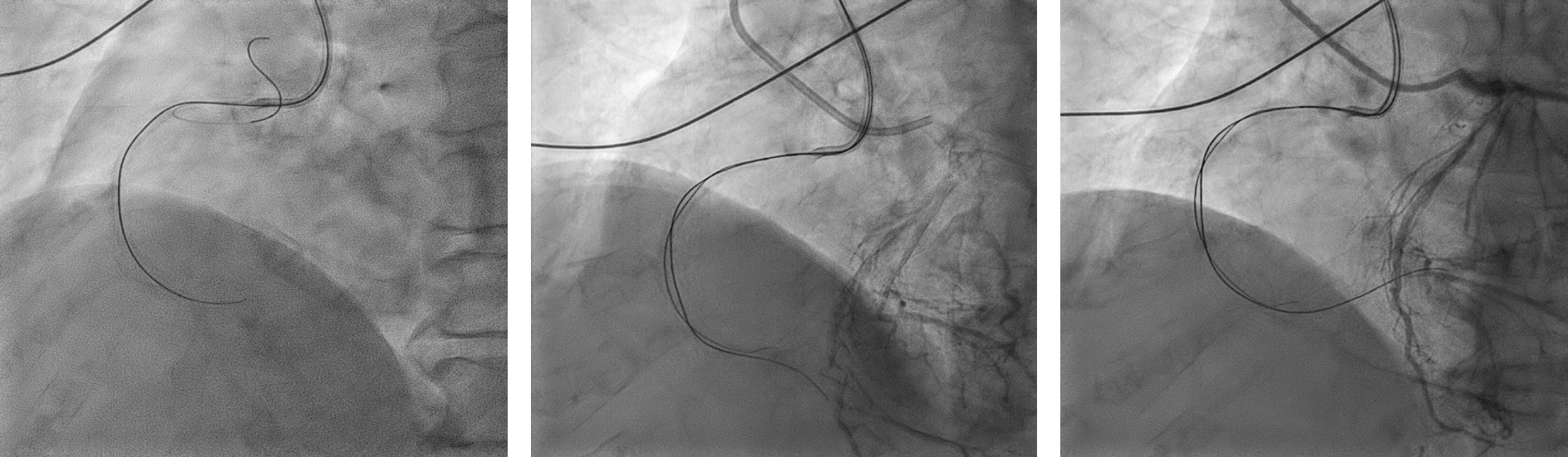
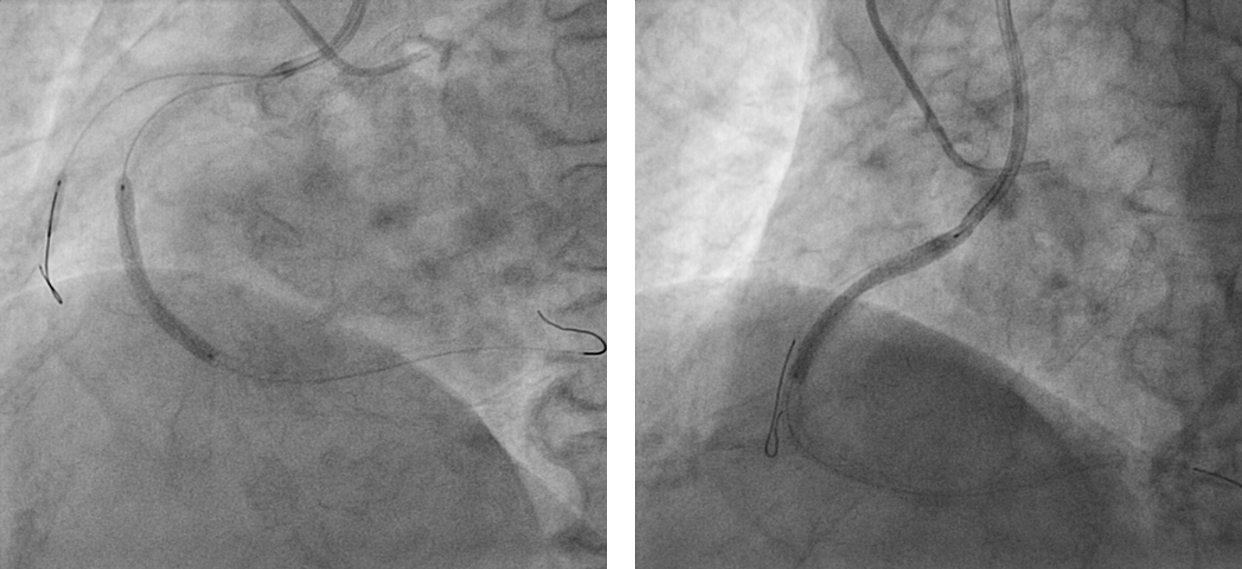
We proceeded with PCI to CTO RCA with SAL 1 guiding catheter and finecross. We were unable to cross the CTO lesion with Fielder XT wire, Gaia second. We attempted parallel wiring but failed. Decided to proceed with PCI to Intermediate artery and LAD instead and to re-attempt PCI to CTO RCA later. We have successfully done PCI to intermediate artery with DCB SEQUENT PLEASE NEO 2.0X20 mm at 6 atm. We stented LAD lesion with DES 2.75x32 mm and post-dilated with NC balloon 3.0x15 mm at 18 atm. She developed contrast induced nephropathy but it improved with hydration.
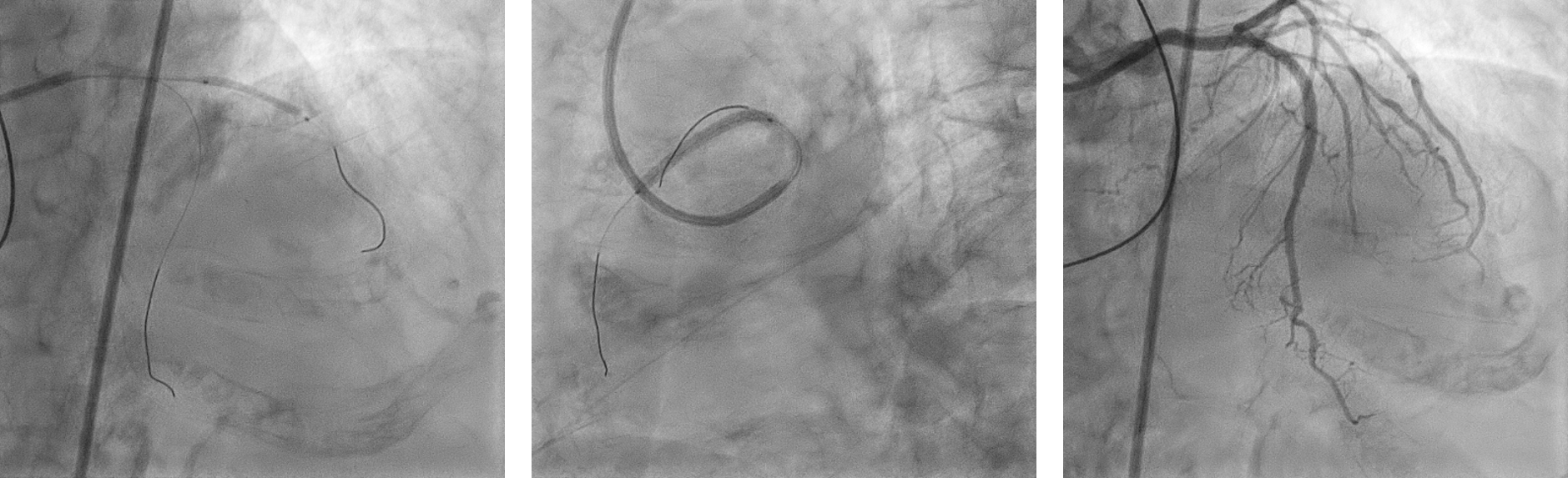
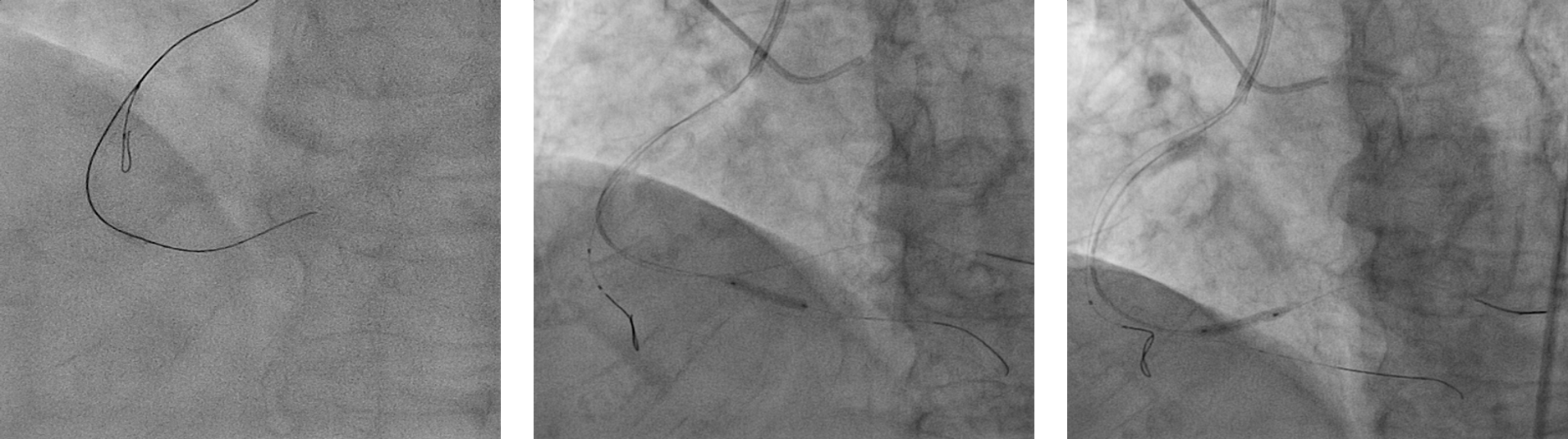
She presented again 3 weeks later with similar chest pain with ECG showing similar changes and echocardiogram showed good EF 58%. We re-attempted PCI to CTO RCA with SAL 1/6R guide with Cosair Pro 150 cm via right femoral and optitorque 5F to left system. We failed to cross the lesion with Fielder XT, Pilot 150 and Conquest Pro 9 and 12. Wires kept going to false lumen. We changed the guide to SAL 1/7F with sideholes and floppy wire to RV branch with anchored balloon. We did ADR with looped Fielder XT-A. Attempted to pass STINGRAY was not successful. We did POBA to distal and mid RCA with 1.5x10 balloon. We were able to pass STINGRAY distally and crossed via ADR to distal RCA with Conquest Pro 12. Exchanged to soft wires and predilatation done. We stented RCA with DES 2.5 x 48 mm, 3.0 x 32 mm and 3.5x 38 mm. Post-dilatation was done with NC 3.5 x 15 mm. We achieved a good result.
Case Summary
It was a case of successful percutaneous coronary intervention to CTO RCA with ADR technique in an elderly patient with multiple comorbidities. We attempted twice with multiple wires including parallel technique. We failed on the first attempt but we successfully crossed for the second time. Failed PCI is not a bad outcome.