
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-104
Presenter
Hannah Byrne
Authors
Hannah Byrne1, Denna Mojuntin2, Faisal Shaikh2
Affiliation
Northampton General Hospital, United Kingdom1, Bedford Hospital, United Kingdom2,
View Study Report
TCTAP C-104
OTHER - Others (Unclassified)
‘Missing the Mark’ - A Case of a Misplaced Central Venous Catheter into the Aortic Arch Despite the Use of Ultrasound Guidance
Hannah Byrne1, Denna Mojuntin2, Faisal Shaikh2
Northampton General Hospital, United Kingdom1, Bedford Hospital, United Kingdom2,
Clinical Information
Patient initials or Identifier Number
MJ
Relevant Clinical History and Physical Exam
A 62-year-old female presented to her local district general hospital (DGH) with a 2-day history of shortness of breath and a productive cough. Previous medical history included chronic obstructive pulmonary disease (COPD), type II diabetes mellitus, hypertension and obesity.
After starting oxygen therapy, her consciousness level deteriorated. She was transferred to intensive care unit (ICU) for non-invasive ventilation and ongoing medical management for treatment of an infective exacerbation of COPD.
After starting oxygen therapy, her consciousness level deteriorated. She was transferred to intensive care unit (ICU) for non-invasive ventilation and ongoing medical management for treatment of an infective exacerbation of COPD.
Relevant Test Results Prior to Catheterization
Admission oxygen saturations were 69% on air and high flow oxygen was administered. Admission bloods: CRP 23, WCC of 15.4, electrolytes and renal function were within normal range. An arterial blood gas revealed a type 2 respiratory failure (pO2 8.19, pCO2 8.14, HCO337.5).
Despite ICU care, she developed septic shock. The patient was mechanically ventilated and inotropic support was required, therefore a central venous catheter (CVC) was inserted.
Despite ICU care, she developed septic shock. The patient was mechanically ventilated and inotropic support was required, therefore a central venous catheter (CVC) was inserted.
Relevant Catheterization Findings
NA
Interventional Management
Procedural Step
A CVC was inserted with ultrasound guidance. The procedure was difficult due to the patient’s large body habitus and although the guidewire appeared slightly kinked upon removal, the line bled back and flushed easily.
A post-procedural chest radiograph demonstrated left lung consolidation, but also raised concerns of CVC misplacement. CVC blood gases were identical to those from an arterial line and arterial waveforms were present when a transducer was connected to the CVC. A CT angiogram of the aortic arch showed the CVC approach the right subclavian artery/crutch of the brachiocephalic trunk and then enter the aortic arch.
An intravenous heparin infusion was commenced and the patient transferred to a tertiary vascular unit.
Endovascular repair was deemed too high risk given the possibility of multiple vessel injuries and complexity of repair. Her significant comorbidities and clinical condition also made her a poor candidate for extraction of the CVC via open surgery with a sternotomy.
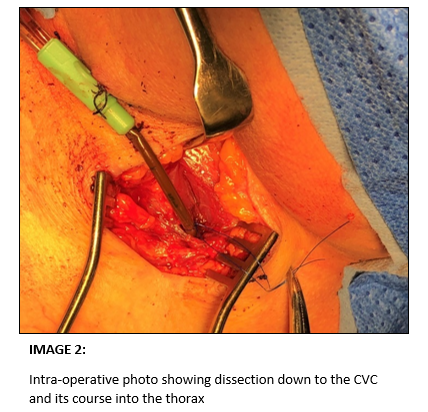
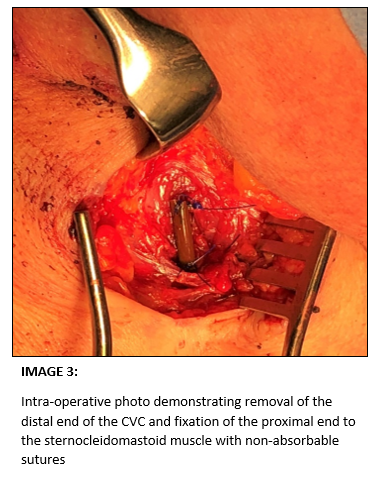
Instead, it was decided the safest surgical approach was to dissect down to the CVC entry point into the thorax, tie it off at this level, then fix and bury the line in the sternocleidomastoid muscle with the aim of it fibrosing over. This operative plan was performed without complications. Following surgery lifelong oral antibiotics and anticoagulation were initiated, in order to prevent the risk of infection or thrombus formation. At 6 month follow up the patient remains well.
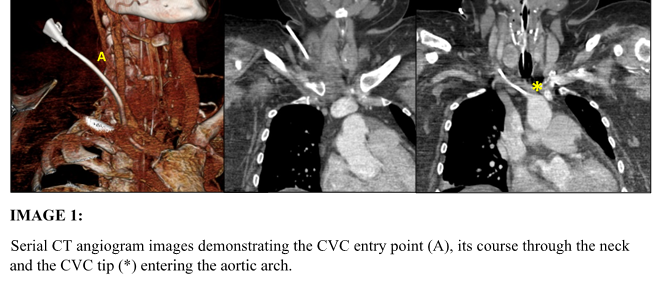
A post-procedural chest radiograph demonstrated left lung consolidation, but also raised concerns of CVC misplacement. CVC blood gases were identical to those from an arterial line and arterial waveforms were present when a transducer was connected to the CVC. A CT angiogram of the aortic arch showed the CVC approach the right subclavian artery/crutch of the brachiocephalic trunk and then enter the aortic arch.
An intravenous heparin infusion was commenced and the patient transferred to a tertiary vascular unit.
Endovascular repair was deemed too high risk given the possibility of multiple vessel injuries and complexity of repair. Her significant comorbidities and clinical condition also made her a poor candidate for extraction of the CVC via open surgery with a sternotomy.
Instead, it was decided the safest surgical approach was to dissect down to the CVC entry point into the thorax, tie it off at this level, then fix and bury the line in the sternocleidomastoid muscle with the aim of it fibrosing over. This operative plan was performed without complications. Following surgery lifelong oral antibiotics and anticoagulation were initiated, in order to prevent the risk of infection or thrombus formation. At 6 month follow up the patient remains well.
Case Summary
CVC malposition is defined as the catheter tip being placed outside of the superior vena cava. Misplacement has been reported in the mediastinum, pleura, pericardium, trachea, oesophagus and subarachnoid space.
Treatment options of CVC iatrogenic arterial injury depend on the patient, clinical situation and extent of vascular injury; however, they include CVC removal and external compression, endovascular repair, or open surgical exploration.
Although rare, vascular complications following CVC insertion can lead to considerable morbidity and mortality. If concerns of iatrogenic arterial injury arise, we recommend leaving the CVC in situ and seeking prompt vascular surgery advice.
Treatment options of CVC iatrogenic arterial injury depend on the patient, clinical situation and extent of vascular injury; however, they include CVC removal and external compression, endovascular repair, or open surgical exploration.
Although rare, vascular complications following CVC insertion can lead to considerable morbidity and mortality. If concerns of iatrogenic arterial injury arise, we recommend leaving the CVC in situ and seeking prompt vascular surgery advice.