
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-033
Presenter
Nanda Iryuza
Authors
Nanda Iryuza1, Doni Firman1, Amir Aziz Alkatiri1,
Affiliation
National Cardiovascular Center Harapan Kita, Indonesia1,
View Study Report
TCTAP C-033
CORONARY - Bifurcation/Left Main Diseases and Intervention
Rescuing Occluded Side Branch During CTO PCI: The Role of Jailed Balloon Technique
Nanda Iryuza1, Doni Firman1, Amir Aziz Alkatiri1,
National Cardiovascular Center Harapan Kita, Indonesia1,
Clinical Information
Patient initials or Identifier Number
Mr. M
Relevant Clinical History and Physical Exam
A 57-years old male with history of NSTEMI one month prior to hospital admission, was planned to undergo elective PCI. The patient was diabetic and hypertensive. At the time of PCI, there was no chest pain, blood pressure was 143/89 mmHg, and other physical examinations were within normal limit.
Relevant Test Results Prior to Catheterization
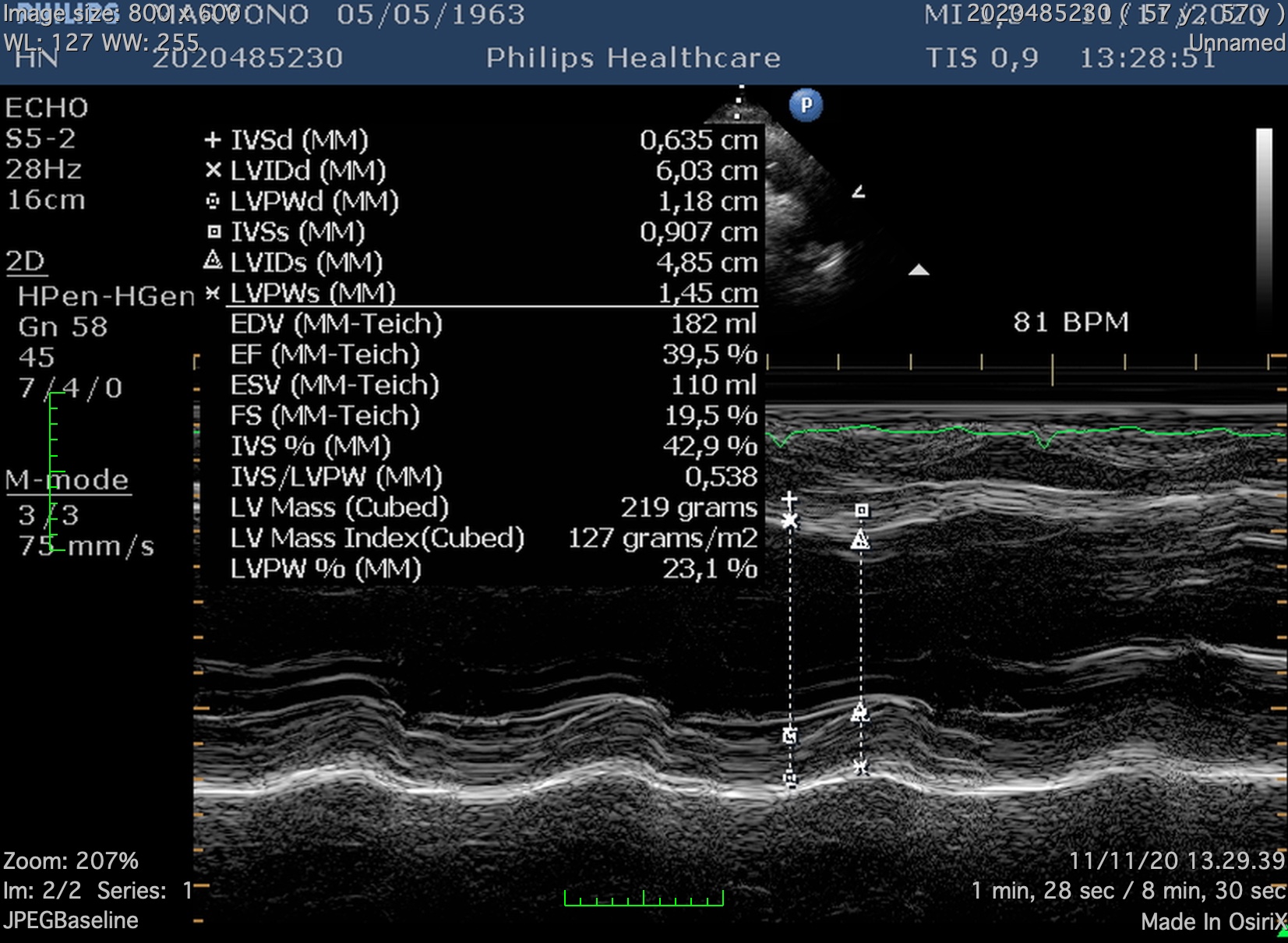
ECG showed normal sinus rhythm with pathological Q wave at anterior and inferior leads. Echocardiography revealed reduced left ventricular ejection fraction to 39% with hypokinesia at the apex, and lateral wall. Complete blood count and renal function were normal. However, the blood glucose level was elevated to 330 mg/dL 1 day prior to PCI, and decreased to 148 mg/dL after continuous insulin injection.
 echo 4c.mov
echo 4c.mov
Relevant Catheterization Findings
Left main: Normal
diagnostic cranial.mov
diagnostic LCA.mov
RCA diagnostic 1.mov
Interventional Management
Procedural Step
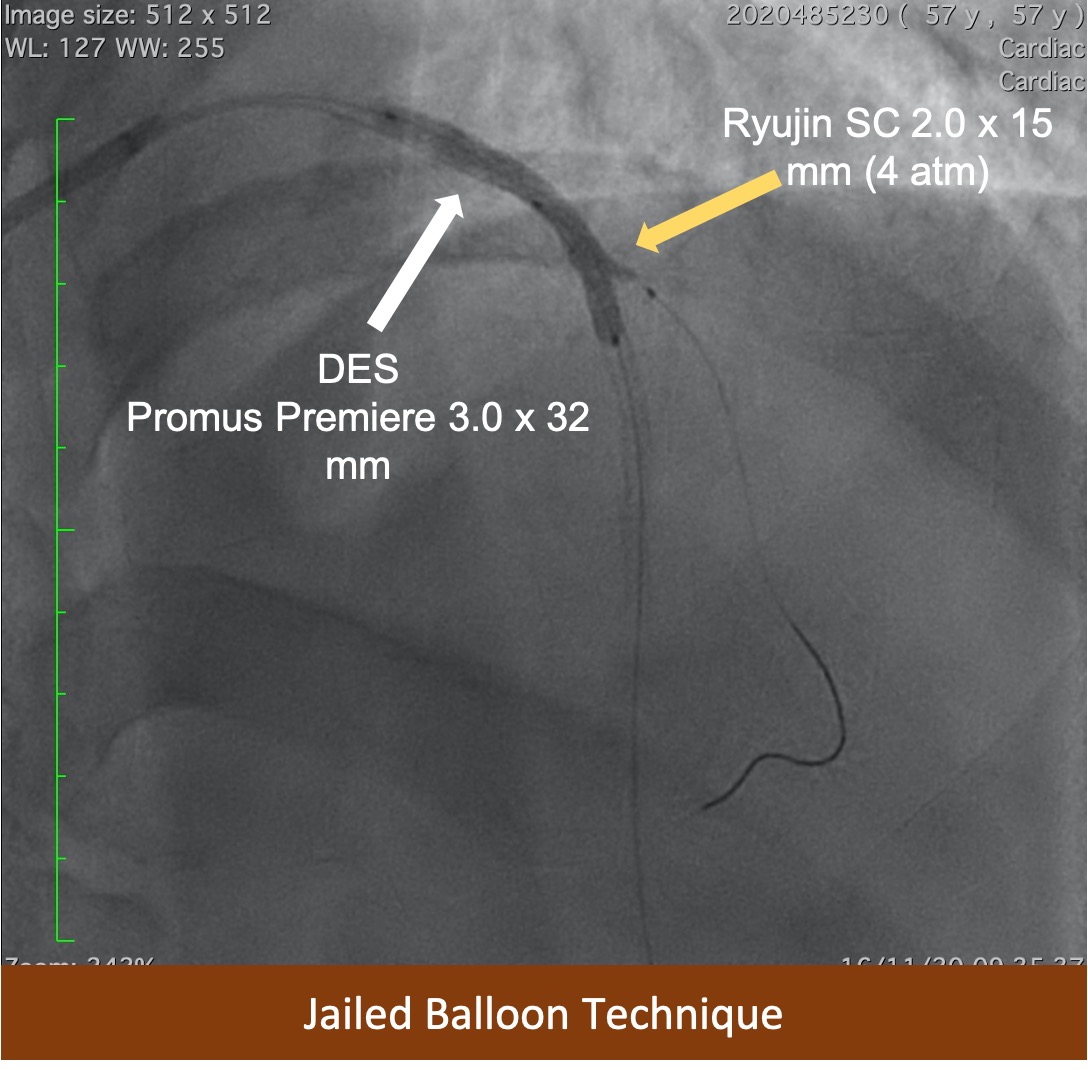
XB 3.5/6F guiding catheter was engaged to LCA. Fielder XTA wire could cross the CTO lesion at the proximal LAD with Finecross Microcatheter back up. Fielder XTA wire exchanged with Runthrough Floppy wire to distal LAD. Pre-dilatation of distal to proximal LAD using 2.0 x 15 mm Ryujin SC balloon with maximum pressure of 12 atm. Angiography revealed non-flow-limiting dissection at mid LAD, and large territory of D2 branch. Another Runthrough wire advanced to distal D2 to preserve the branch. First Xience Prime 2.5 x 33 mm DES deployed at the mid to distal LAD at 8 atm, and the balloon-stent was used to pre-dilate the mid and proximal LAD. Angiography showed TIMI 3 flow to distal LAD, however, the large D2 branch was compromised. Jailed balloon technique was applied to rescue the D2 branch by inserting 2.0 x 15 mm SC Ryujin balloon and inflated to 4 atm at the proximal D2 before it was retracted proximally to bifurcation of LAD-D2. The balloon was inflated at 4 atm, simultaneously the second DES Promus Premier 3.0 x 32 mm was inflated to 12 atm at proximal to mid LAD. Jailed wire at D2 branch was removed, and angiography showed TIMI 3 flow to distal LAD, and the D2 branch was opened. POT performed from mid to proximal LAD proximal to D2 branch. Final angiography revealed TIMI 3 flow with no dissection, and no side branch occlusion.
post lesion prep_1st DES.mov
Final 1.mov
Case Summary
Provisional single stent strategy is preferable over two stent strategy in terms of treating most of bifurcation lesions. However, there is a risk of side branch compromise once the stent placed at the main vessel. Jailed balloon technique is proven to be safe and beneficial in provisional single stent strategy to avoid the side branch impairment and even rescuing the occluded side branch after main vessel stent deployment in coronary bifurcation lesions.