
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-111
Presenter
Faizal Khan Abdullah
Authors
Faizal Khan Abdullah1, Shaiful Azmi Yahaya1, Kumara Gurupparan Ganesan1, Jayakhanthan Kolanthaivelu2, Wan Faizal Bin Wan Rahimi Shah1, Afif Ashari1, Faten Aqilah Aris1
Affiliation
National Heart Institute, Malaysia1, Cardiovascular Sentral Kuala Lumpur, Malaysia2,
View Study Report
TCTAP C-111
STRUCTURAL HEART DISEASE - Valvular Intervention: Aortic
Calcified Descending Aortic Dissection During TAVI
Faizal Khan Abdullah1, Shaiful Azmi Yahaya1, Kumara Gurupparan Ganesan1, Jayakhanthan Kolanthaivelu2, Wan Faizal Bin Wan Rahimi Shah1, Afif Ashari1, Faten Aqilah Aris1
National Heart Institute, Malaysia1, Cardiovascular Sentral Kuala Lumpur, Malaysia2,
Clinical Information
Patient initials or Identifier Number
KHH
Relevant Clinical History and Physical Exam
76 year old /Female
On Examination
On Examination
Relevant Test Results Prior to Catheterization
Echocardiogram: Left ventricular ejection fraction 62%, mildly dilated left atrium, severe aortic stenosis with AVA 0.66cm, mean PG: 51mmHgMax PG: 91mmHgMild Aortic regurgitation
ECG: Sinus rhythm
 echo.mpg
echo.mpg
ECG: Sinus rhythm
Relevant Catheterization Findings
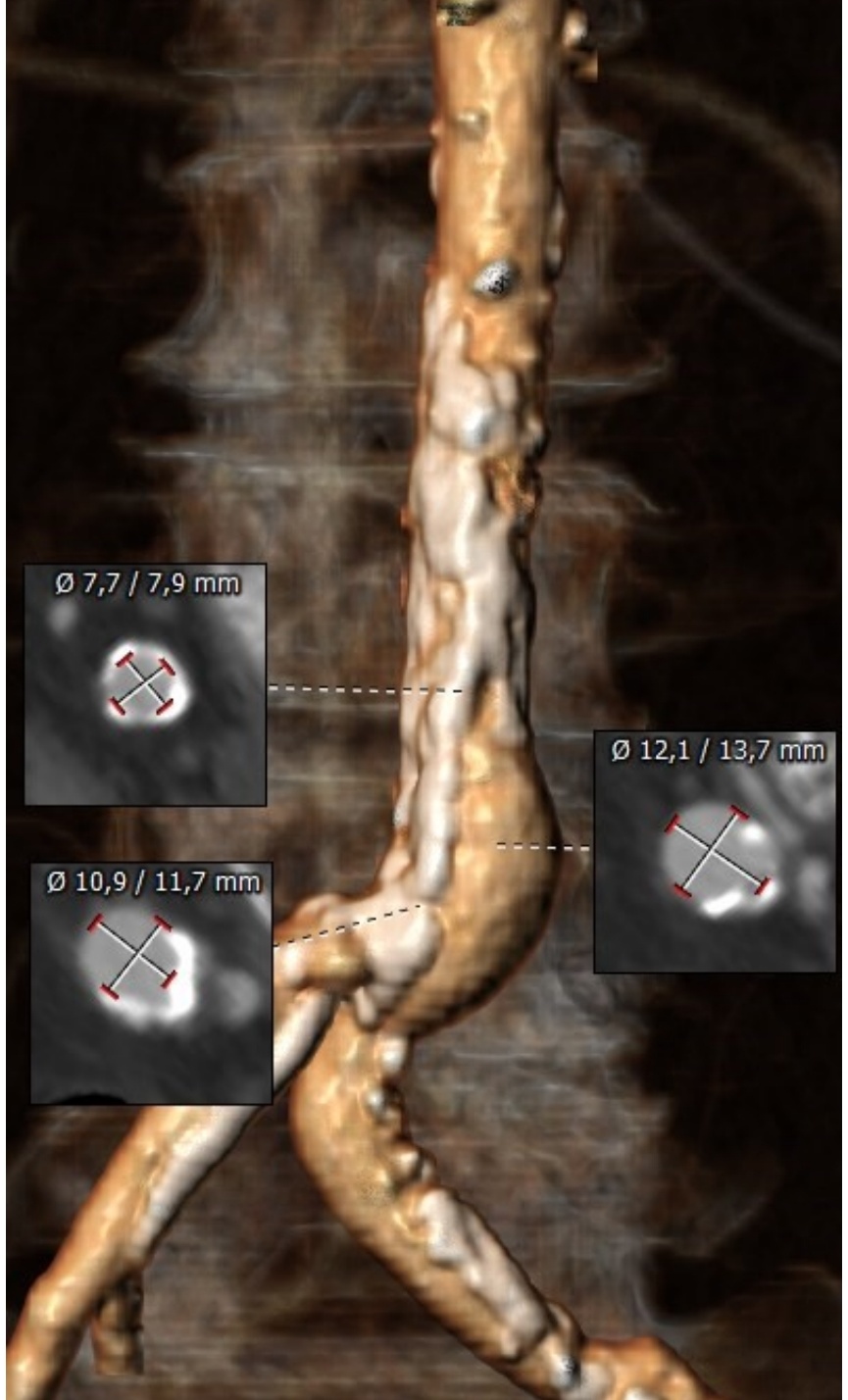
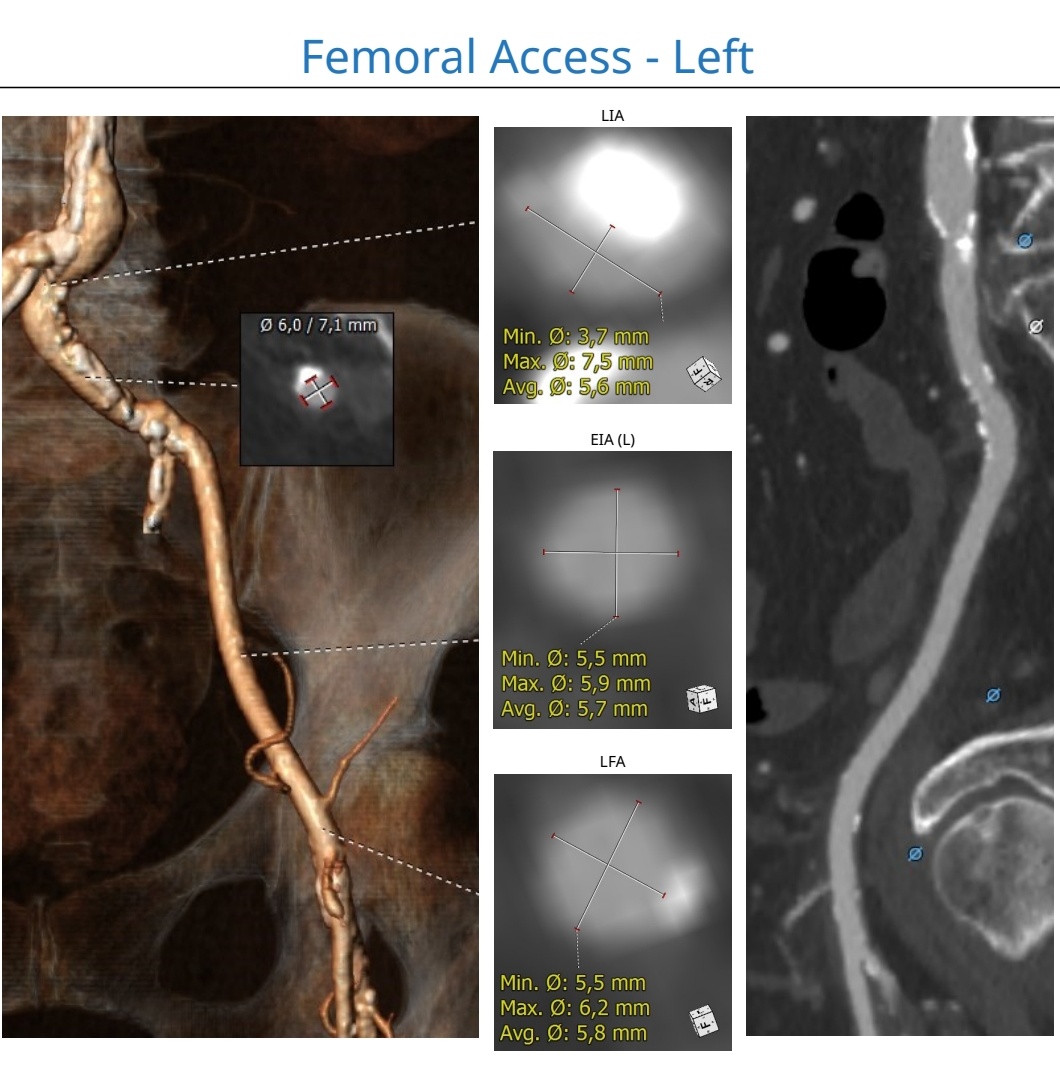
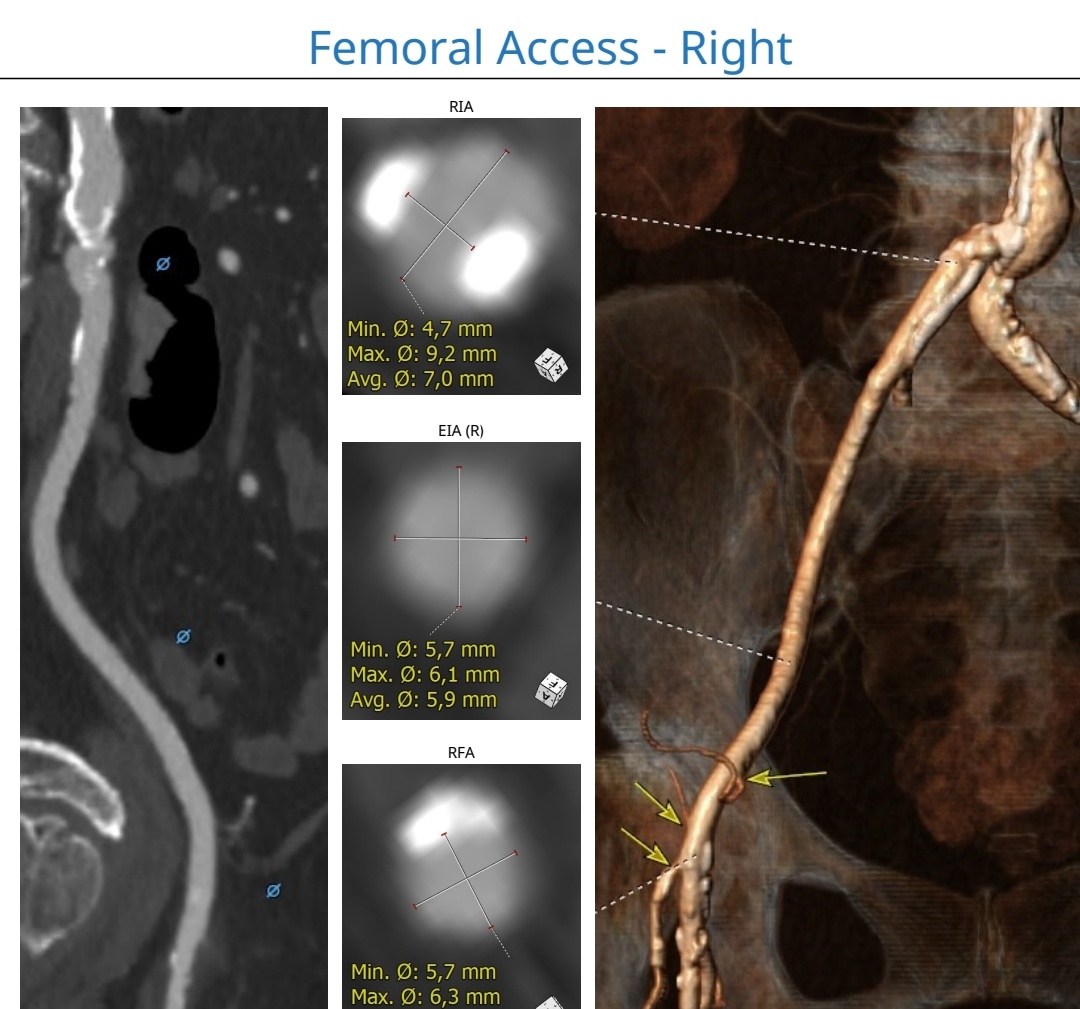
Graft Study: All grafts patentBilateral iliac artery calcification, left iliac worse calcificationRight iliac ostium size: 4.7 mm x 9.2 mm, 2 point calcificationLeft iliac ostium size: 3.7 mm x 7.5 mmDistal aorta calcification: Lumen size 7.7 mm x 7.9mm, calcification
Interventional Management
Procedural Step
Bilateral femoral puncture with 6F sheath. Preclosed with 2x proglide on right femoral.
TAVI sheath cant go in.mpg
Calcium dissect.mpg
post dissect.mpg
Case Summary
Aorta calcification is commonly seen especially in the elderly where the most common age group TAVI being performed. In this case, there is a severe calcification at distal aorta which was underestimated. Though the initial report showed there is enough space for the TAVI device to go through, the extent of calcium was extensive that it didn't allow the device to go through despite of predilatation.Pushing any large device across a severe calcification need to be made carefully as stripping of calcium could lead to life-threatening aorta perforation. In this case, we were fortunate that calcium stripping only caused non flow limiting dissection.