
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-100
Presenter
Vicknesan Kulasingham
Authors
Vicknesan Kulasingham1, Mahadevan Gurudevan2, Heng Shee Kim3, Kim Fong Ng3, Hazrini Abdullah4, Tee Choon Keong3, Kumutha Gobal3, Adelyn Nisha Henry3
Affiliation
Ministry of Health Malaysia, Malaysia1, Sultanah Amina Hospital, Malaysia2, Sultanah Aminah Hospital, Malaysia3, Hospital Sultanah Aminah, Malaysia4,
View Study Report
TCTAP C-100
IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Non-Invasive
Myocardial Infarction with Non-obstructive Coronary Arteries (MINOCA)
Vicknesan Kulasingham1, Mahadevan Gurudevan2, Heng Shee Kim3, Kim Fong Ng3, Hazrini Abdullah4, Tee Choon Keong3, Kumutha Gobal3, Adelyn Nisha Henry3
Ministry of Health Malaysia, Malaysia1, Sultanah Amina Hospital, Malaysia2, Sultanah Aminah Hospital, Malaysia3, Hospital Sultanah Aminah, Malaysia4,
Clinical Information
Patient initials or Identifier Number
Mr NS
Relevant Clinical History and Physical Exam
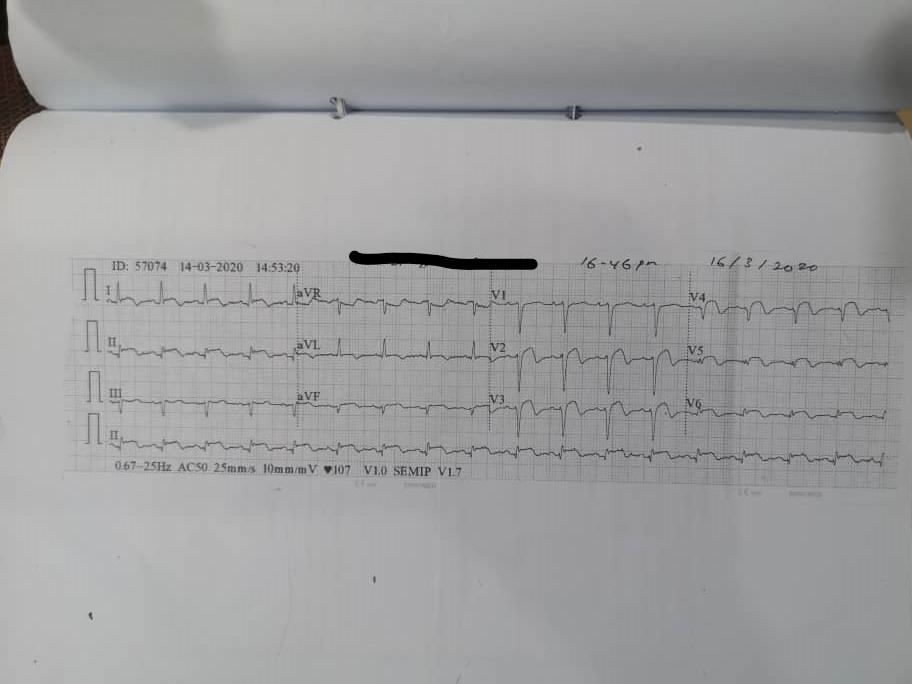
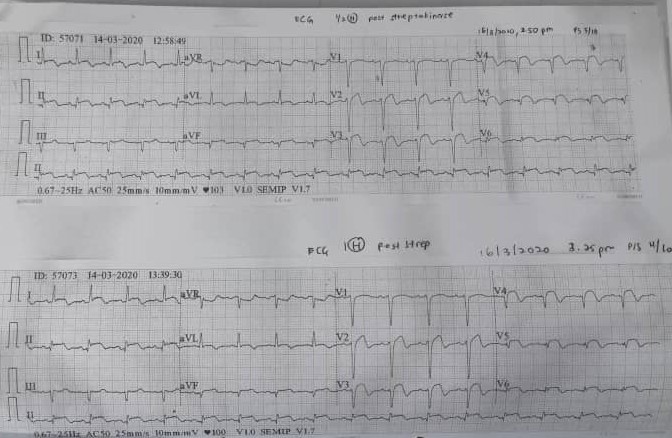
26 years old gentleman, active smoker presented with chest pain for 2 days. He has no known medical illness. In the ED, his vitals was stable and no signs of heart failure. 1st ECG showed ST elevation and he was thrombolysed. He was then admitted to CCU. He started having fever with intermittent chest pain. ECG did not show complete resolution. Our differential diagnosis at this point was acute myopericarditis, for which a CMR was done.
Relevant Test Results Prior to Catheterization
Haemoglobin 153g/dL (130-170 g/L), white cell counts 21.5x10^9/L(4-10x10^9/L), platelets count 244x10^9/L (150-410x10^9/L). Sodium 134mmol/L,potassium 3.69mmol/L, Chloride 96mmol/L, urea 3.5mmol/L, creatinine83micromol/L, creatinine kinase 1085mmol/L, Troponin T 4048pg/nl, CRP 197mg/dl.
Chest X-ray: Clear lung fields
ECG: SR, ST elevation inferior leads, Deep TWI and Q waves anterior leads.
Echocardiography: LVEF 50% with apical hypokinesia. No Clot or thrombus seen.
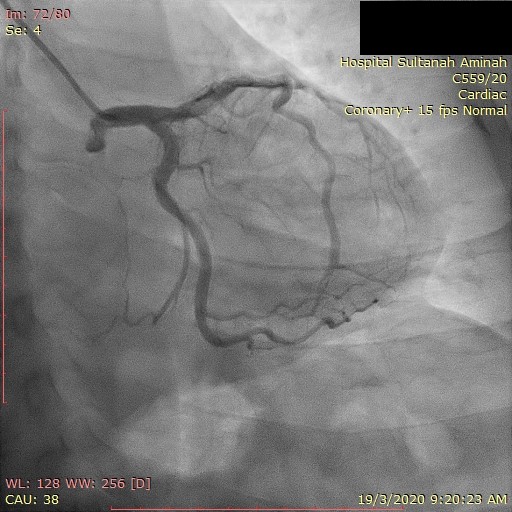
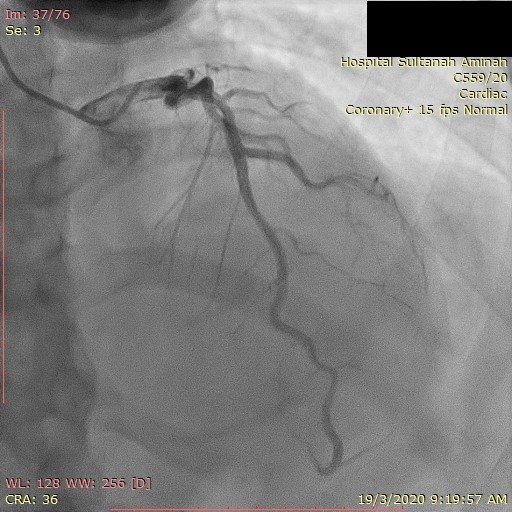
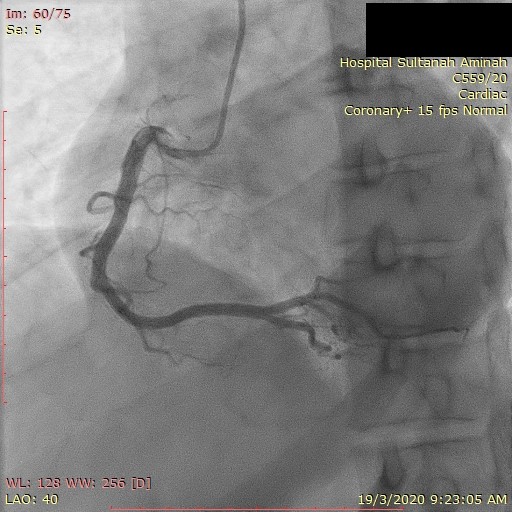
Relevant Catheterization Findings
Coronary angiogram showed minor CAD with mLAD stenosis of 20%.
Interventional Management
Procedural Step
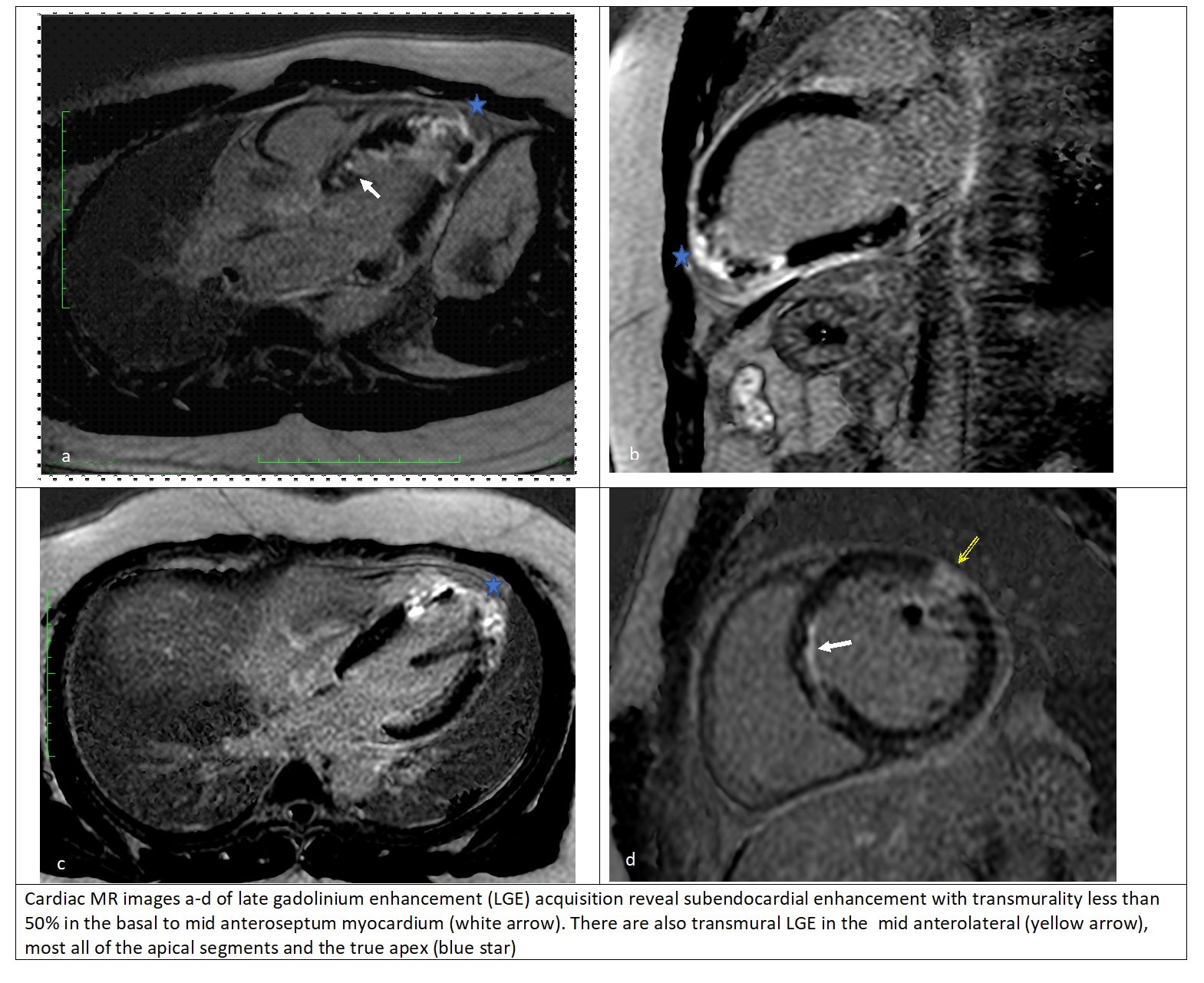
Cardiac MRI Sequences: BB multislice, WB multislice,Cine 2C,3C,4C,STIR,RVOT,SA,EGE and LGELeft ventricle: Mildly dilated LV cavity with mild LVSD EF49%. Mid to apical anteroseptal, anterior and anterolateral dyskinesia. Normal LV Mass index. STIR images shows hyperintensities involving the mid anteroseptal and mid anterolateral segments.Right ventricle: Normal RV cavity and normal RV function with RVEF 57%.No RVH or RWMA.Atria: Normal LA 25mls/m2.Normal RA 21mls/m2Valves: Aortic valve is trileaflet and opens well. Mild MR with regurgitant volume of 11mls and regurgitant fraction of 13%Great vessels: thoracic aorta and pulmonary artery is of normal calibre. No coarctation.Pericardium: normal pericardium thickness, no pericardial effusion.Gadolinium study: Early phase there is a small apical thrombus measuring 1.43cmx0.5cm. No microvascular obstruction. Late phase there is subendocardial LGE mid-anteroseptal <50%, mid anterolateral full thickness, apical septal and lateral full thickness and apical inferior <50%. This is in keeping with prior infarction LAD territory(2 segments viable, 1segment non viable) and LCX/RCA territory (2 segements non viable).Above features are in keeping with Ischaemic Cardiomyopathy.
Case Summary
MINOCA is defined as myocardial infarction with non obstructing coronaries (stenosis <50%). MINOCA is seen in about 5%-6% of AMI patients and demographics for MINOCA are slightly different from obstructive CAD. MINOCA is usually a working diagnosis with various possible etiology which could be coronary causes or non-coronary causes. Challenges faced in MINOCA are diagnosis and imaging like cardiac MRI plays a very important role. Treatment of MINOCA is also a challenge as there is not much evidence on the effectiveness of the conventional treatment for AMI.