
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-098
Presenter
Ayan Kar
Authors
Debdatta Bhattacharyya1, Ayan Kar2, Kishan Kumar Agarwal2, Snehil Goswami3
Affiliation
RN Tagore Hospital, India1, NH-Rabindranath Tagore International Institute of Cardiac Sciences, India2, NH MMI Hospital, India3,
View Study Report
TCTAP C-098
IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular
Use of Intravascular Lithotripsy in Calcium Management: Comparison of Intravascular Ultrasound and Optical Coherence Tomography Guidance
Debdatta Bhattacharyya1, Ayan Kar2, Kishan Kumar Agarwal2, Snehil Goswami3
RN Tagore Hospital, India1, NH-Rabindranath Tagore International Institute of Cardiac Sciences, India2, NH MMI Hospital, India3,
Clinical Information
Patient initials or Identifier Number
PG,RKR
Relevant Clinical History and Physical Exam
1. Patient PG71 years old Diabetic Hypertensive, post PTCA to LAD 2010now presents with unstable angina
2. Patient RKR66 years hypertensive CKD on MHD presented with unstable anginaA known patient of Chronic kidney Disease on twice a week maintenance hemodialysis
 PG RCA first CAG.avi
PG RCA first CAG.avi
2. Patient RKR66 years hypertensive CKD on MHD presented with unstable anginaA known patient of Chronic kidney Disease on twice a week maintenance hemodialysis
Relevant Test Results Prior to Catheterization
1. Patient PGHemoglobin:11.2 g/dlcreatinine:1.2 mg/dlFBS:102 mg/dlEcho: hypokinetic inferior wall ,EF 50%
2.Patient RKRHemoglobin:9.0 g/dlCreatinine:7.82 mg/dlEcho: normal LV function EF 62%
RK ROY 1st look CAG.avi
2.Patient RKRHemoglobin:9.0 g/dlCreatinine:7.82 mg/dlEcho: normal LV function EF 62%
Relevant Catheterization Findings
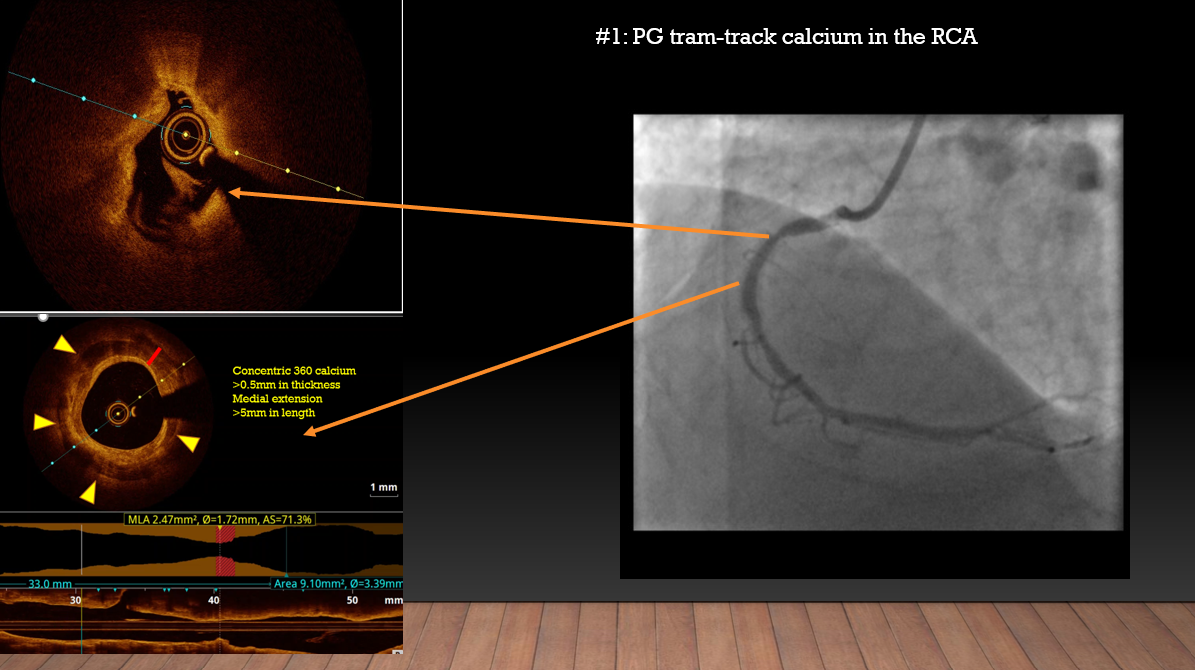
Patient 1 PG:LMCA: normalLAD: Ostial 80% with another discrete calcific lesion in the mid LAD with 70% stenosisLCX: Non-dominantRCA: long segment calcific disease in the proximal mid RCA with tight 80% disease in the proximal part
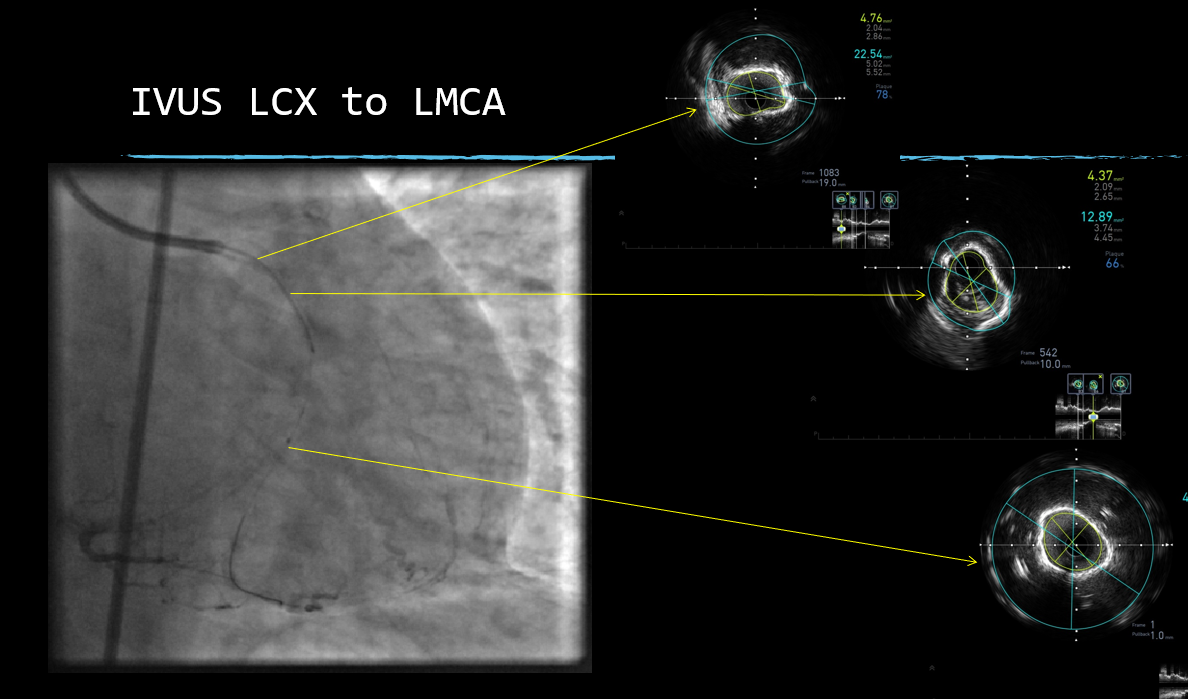
Patient 2 RKR:LMCA: normal LAD: long segment calcific non-obstructive disease in the the LADLCX: dominant long segment calcific disease involving proximal part with maximum diameter stenosis of 70%RCA: non dominant minor plaques
PG RCA Final Result.avi
RKR final result.avi
Patient 2 RKR:LMCA: normal LAD: long segment calcific non-obstructive disease in the the LADLCX: dominant long segment calcific disease involving proximal part with maximum diameter stenosis of 70%RCA: non dominant minor plaques
Interventional Management
Procedural Step
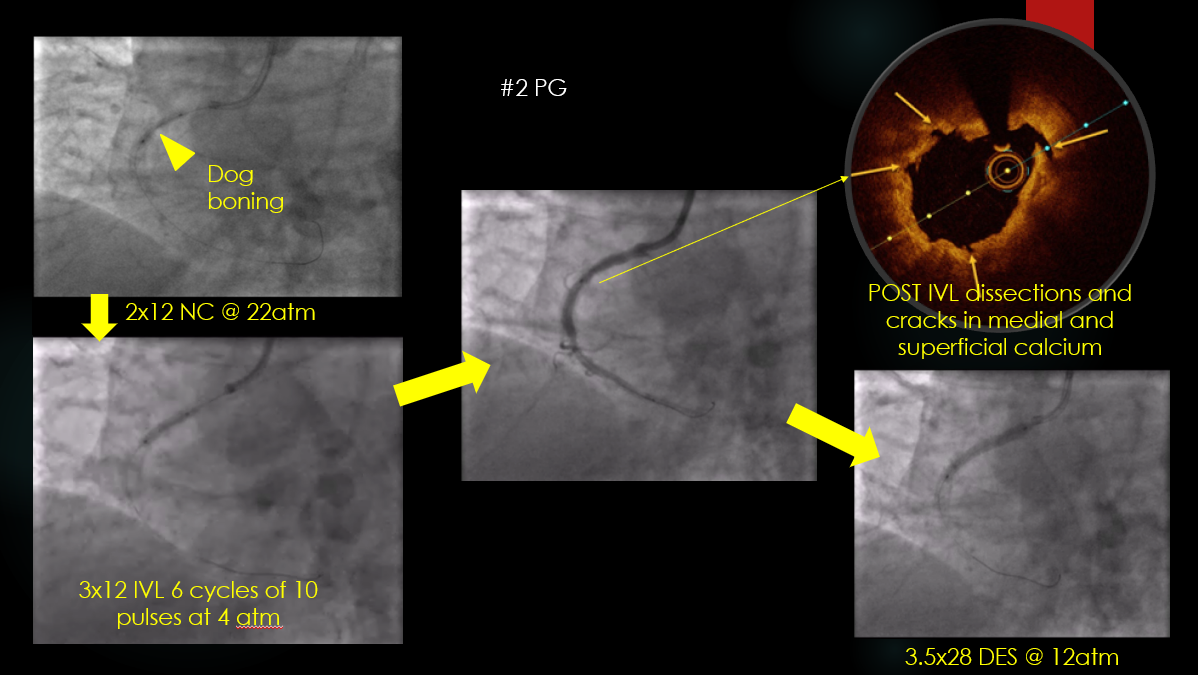
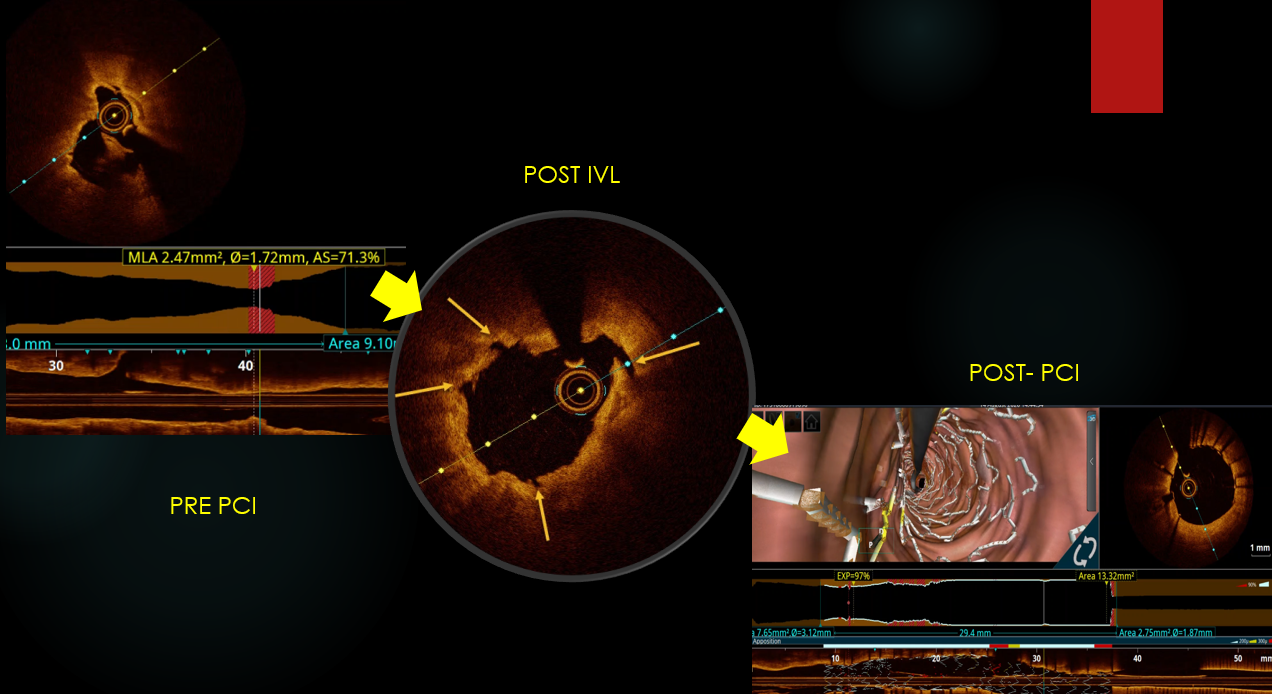
Procedure #1 PGRCA wired with 0.014 Runthrough intermediate wire, Pre-dilatation with a 2.5x12 NC at 22 atm produced a persistent waist. OCT interrogation to the RCA showed long segment concentric >1 mm depth medial calcification with the tightest zone showing significant luminal compromise.3x 12 IVL balloon was inflated to 4 atm and 6 cycles of 10 pulses were delivered until full expansion in IVL balloon was noted with disappearance of waist. Post IVL OCT showed multiple cracks extending into the medial calcium .RCA was stented with 3.5x28mm DES followed by a post dilatation with 3.5x12mm at 22atm. Post PCI OCT showed adequate stent expansion and apposition and no evidence of edge dissection.
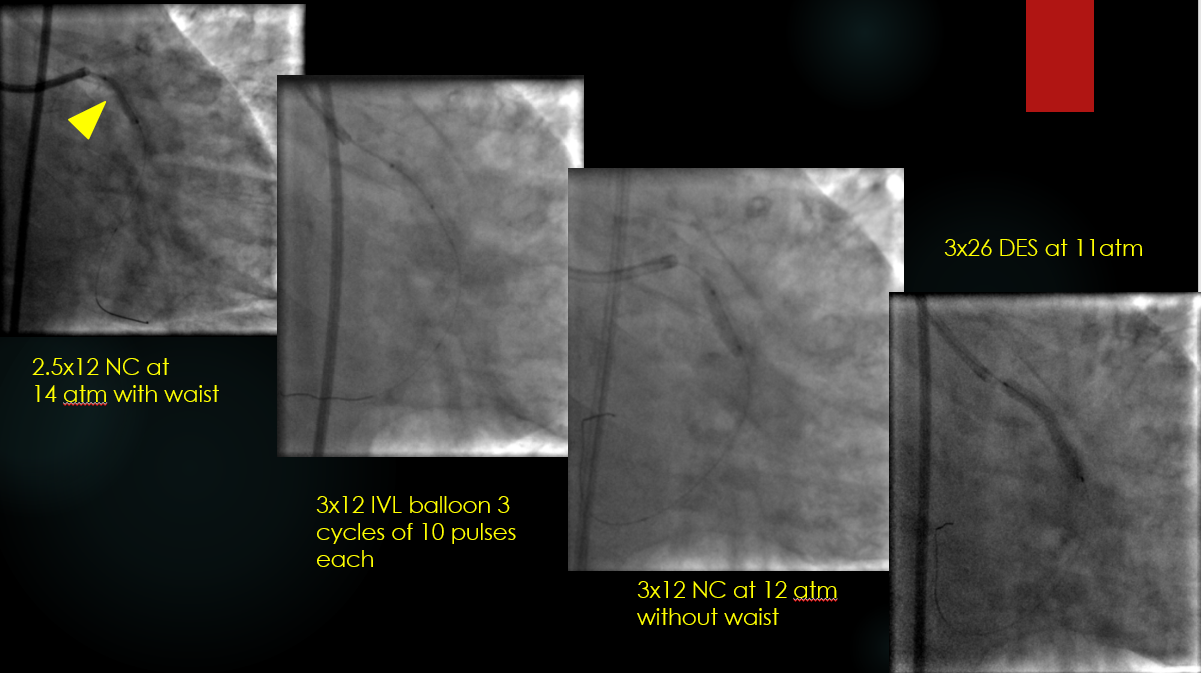
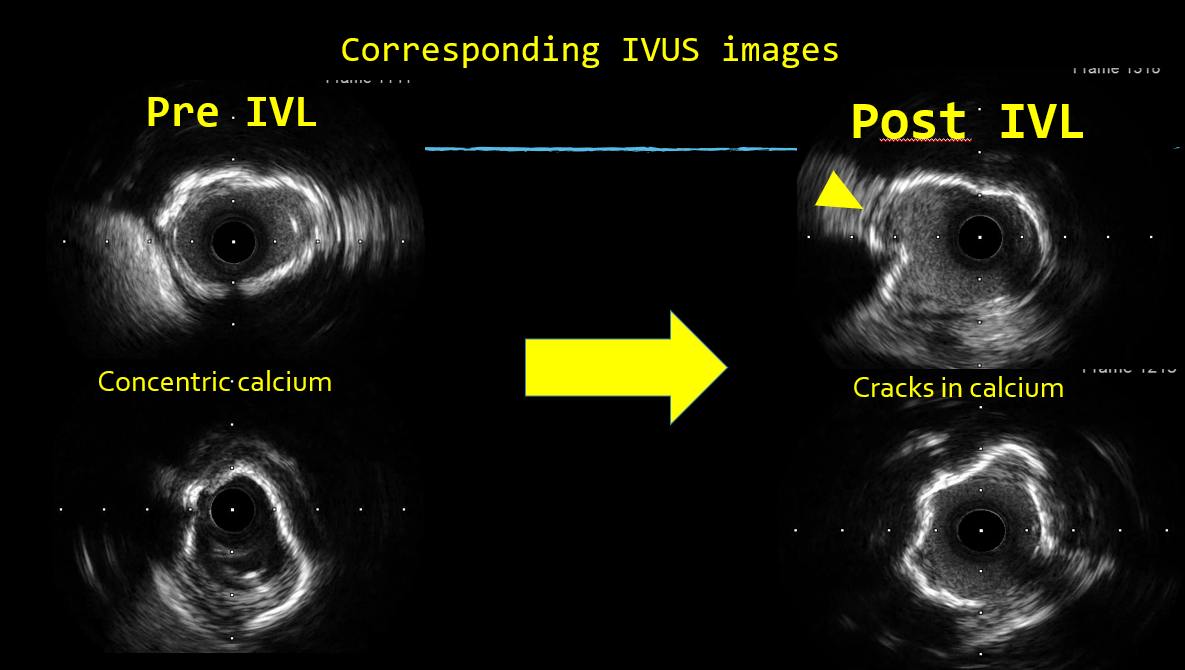
Procedure #2 RKRLCX was wired with Whisper Extra Support wire, and the lesion was pre-dilated with 2.5x12 balloon at 20atm with a significant persistent waist.IVUS interrogation was done to the LCX which shows>270 degree arc of calcium with tight proximal disease, 3x12mm IVL was inflated at 4 atm.4 cycles of 10 pulses each were delivered following which a 3x26 DES was deployed at 11 atm and post dilated with 3.5x12 NC at 12 to 14 ATM Final IVUS run was done to ensure proper stent deployment and exclude edge dissection
Procedure #2 RKRLCX was wired with Whisper Extra Support wire, and the lesion was pre-dilated with 2.5x12 balloon at 20atm with a significant persistent waist.IVUS interrogation was done to the LCX which shows>270 degree arc of calcium with tight proximal disease, 3x12mm IVL was inflated at 4 atm.4 cycles of 10 pulses each were delivered following which a 3x26 DES was deployed at 11 atm and post dilated with 3.5x12 NC at 12 to 14 ATM Final IVUS run was done to ensure proper stent deployment and exclude edge dissection
Case Summary
Intravascular lithotripsy is a new and effective mode of calcific plaque modification. Intravascular imaging is necessary to assess these lesions prior to usage of IVL. Not only does it help in confirming the exact location of calcium in the vessel wall, whether subintimal or a little deeper, it also shows the arc of calcium, the length of the vessel involved and in case of OCT also the thickness of the calcific plaque. After IVL it also demonstrates the cracks in the calcium very clearly, more so in the case of OCT and gives confidence to the operator that stent deployment would now be successful.The above mentioned cases demonstrate the utility of both IVUS and OCT in such situations.