
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-016
Presenter
Siti Dalila Adnan
Authors
Siti Dalila Adnan1, Nor Halwani Habizal2, Kamaraj Selvaraj3, Asri Ranga3, Abd Kahar Abd Ghapar3
Affiliation
Serdang Hospital, Malaysia1, Hospital Sultan Idris Shah Serdang, Malaysia2, Sultan Idris Shah Serdang Hospital, Malaysia3,
View Study Report
TCTAP C-016
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
A Case of Successful Rotational Atherectomy in a Dissected and Ectatic Right Coronary Artery
Siti Dalila Adnan1, Nor Halwani Habizal2, Kamaraj Selvaraj3, Asri Ranga3, Abd Kahar Abd Ghapar3
Serdang Hospital, Malaysia1, Hospital Sultan Idris Shah Serdang, Malaysia2, Sultan Idris Shah Serdang Hospital, Malaysia3,
Clinical Information
Patient initials or Identifier Number
SD01046128
Relevant Clinical History and Physical Exam
A 76-year-old male, ex-smoker with a past medical history of Ischemic Heart Disease. Cardiovascular risk factors including Type II Diabetic Mellitus, Hypertension, Coronary Artery Disease, Cerebro Vascular Accident (CVA)He presented with sudden onset of crushing chest pain associated with exertional dyspnoea.Clinical examination.:Blood pressure 123/65 mmHg Heart rate of 88/minCardiovascular and respiratory system were unremarkable.No other abnormalities in other systemic physical examination.
Relevant Test Results Prior to Catheterization
Renal Profile: Urea 4.8, Na 142, K 3.8, Creatinine 114FBC: Hb 15.1, WCC 8.5, Platelet 271Echocardiogram: demonstrated a left ventricular function of 65% with no regional wall motion hypokinesiaElectrocardiogram (ECG) showed regular sinus rhythm, with ST segment depression at inferior leads
Relevant Catheterization Findings
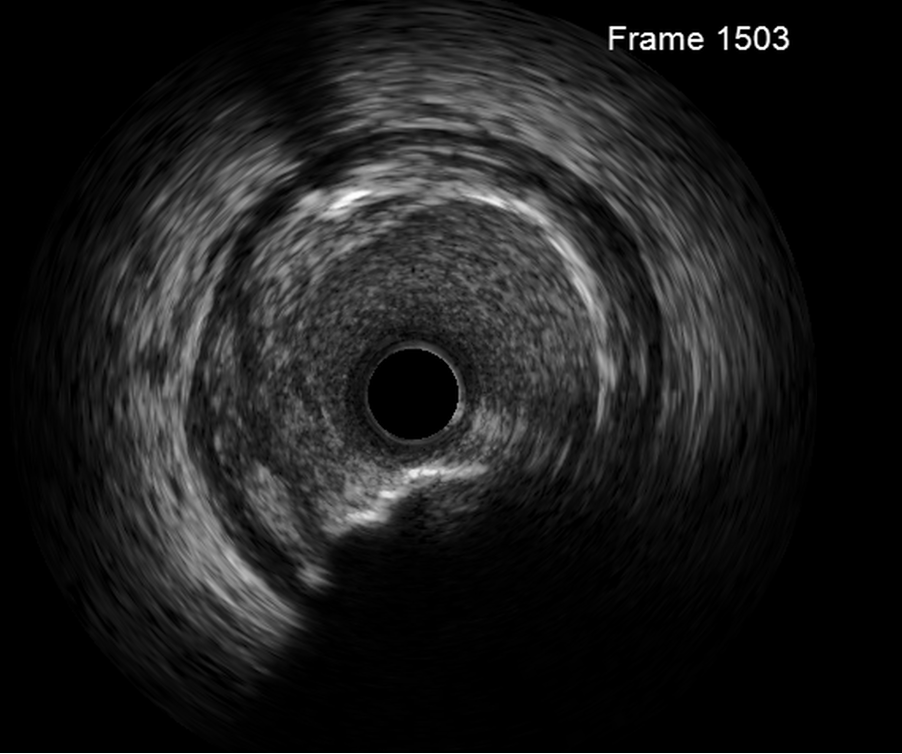
LM: no significant stenosisLAD: Ostial LAD 50% stenosis, mid to distal LAD moderate diseaseLCX: Ectatic vessel, proximal to mid LCX moderate 60-70%, distal LCX and OM bifurcation lesion, CTO at OM1RCA: Ectatic and Calcified vessel with multiple tandem lesion from distal to proximal RCA causing 70-90% stenosis.Presence of thin line dissection at proximal RCA, TIMI 3 flow, which was further confirmed with IVUS images. Noted dissection of calcified plaque extending into tunica media, no flap.
 rca1.avi
rca1.avi
Interventional Management
Procedural Step
Radial approach with 6Fr JR3.5 guiding catheterTransvenous temporary pacemaker inserted via right femoral vein, anticipating transient bradycardia during RCA intervention Run-through floppy with fine cross micro catheter wired into RCA.Proceed with rota 1.7 burr, 160K RPM
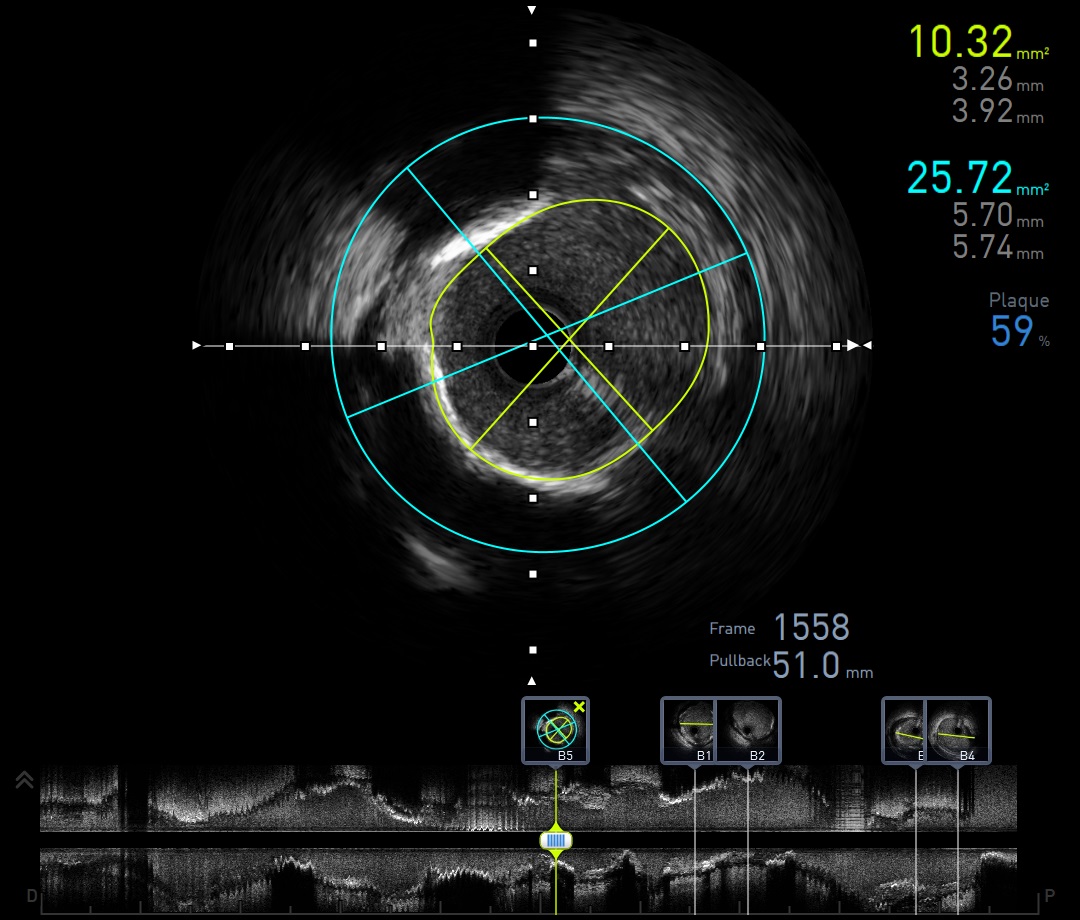
IVUS
Predilated with :- dRCA-ostialRCA Sapphire NC 3.5x15mm at 16-20 ATM- dRCA-ostialRCA Scoreflex 3.5x15mm at 14 ATM
Stented with :- distal-midRCA Onyx 4.5x30mm at 12 ATM- midRCA-pRCA Onyx 4.5x26mm at 12 ATM- proxRCA-ostialRCA Onyx 4.5x18mm at 12-16 ATM
Postdilated with :- distalRCA-ostialRCA with Sapphire NC 4.5mmx15mm at 16-20 ATM, Ostial flare done 20ATM
IVUS post
Well opposed stent, no dissection
postpci.avi
IVUS
| Segment | MLA (mm2) | Lumen diameter (mm) | Vessel diameter (mm) | Plaque Burden (%) |
| Distal RCA | 14.64 | 4.24 / 4.40 | 6.61 / 6.92 | 59 |
| Mid RCA (lesion) | 10.32 | 3.26 / 3.92 | 5.7 / 5.74 | 59 |
Predilated with :- dRCA-ostialRCA Sapphire NC 3.5x15mm at 16-20 ATM- dRCA-ostialRCA Scoreflex 3.5x15mm at 14 ATM
Stented with :- distal-midRCA Onyx 4.5x30mm at 12 ATM- midRCA-pRCA Onyx 4.5x26mm at 12 ATM- proxRCA-ostialRCA Onyx 4.5x18mm at 12-16 ATM
Postdilated with :- distalRCA-ostialRCA with Sapphire NC 4.5mmx15mm at 16-20 ATM, Ostial flare done 20ATM
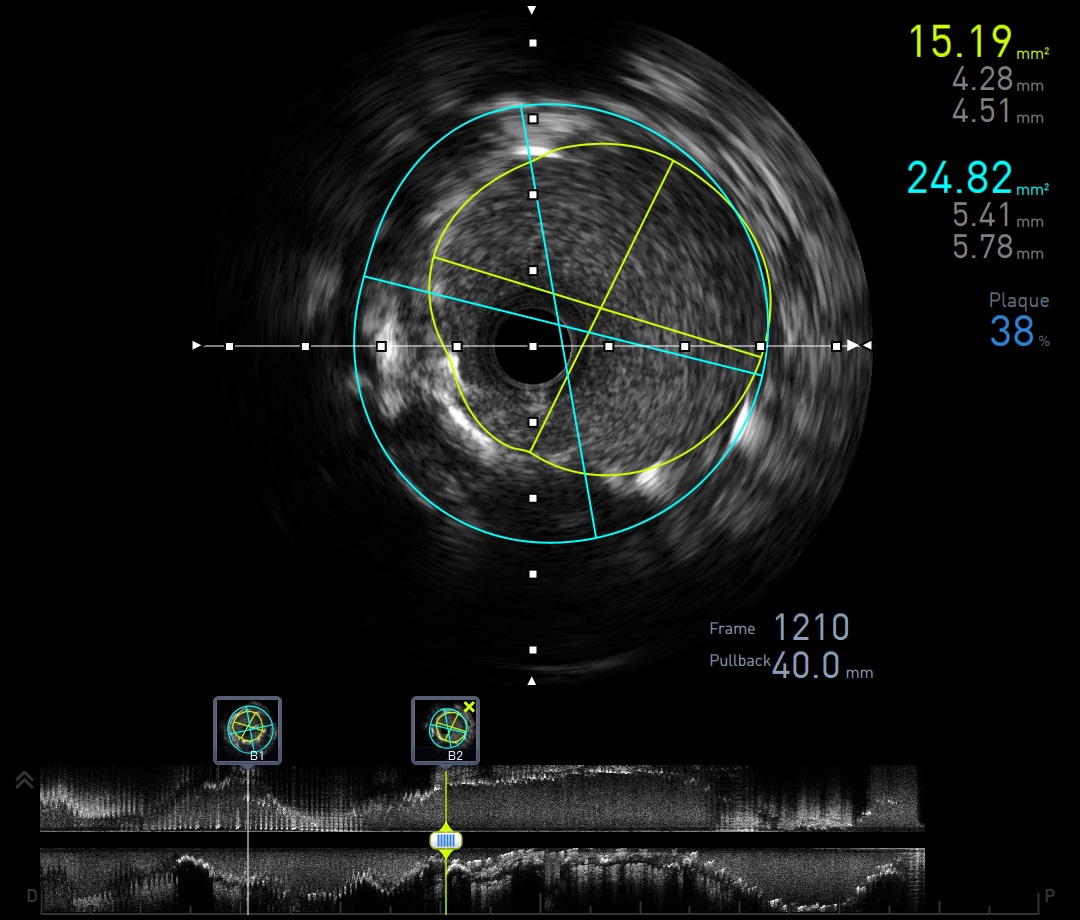
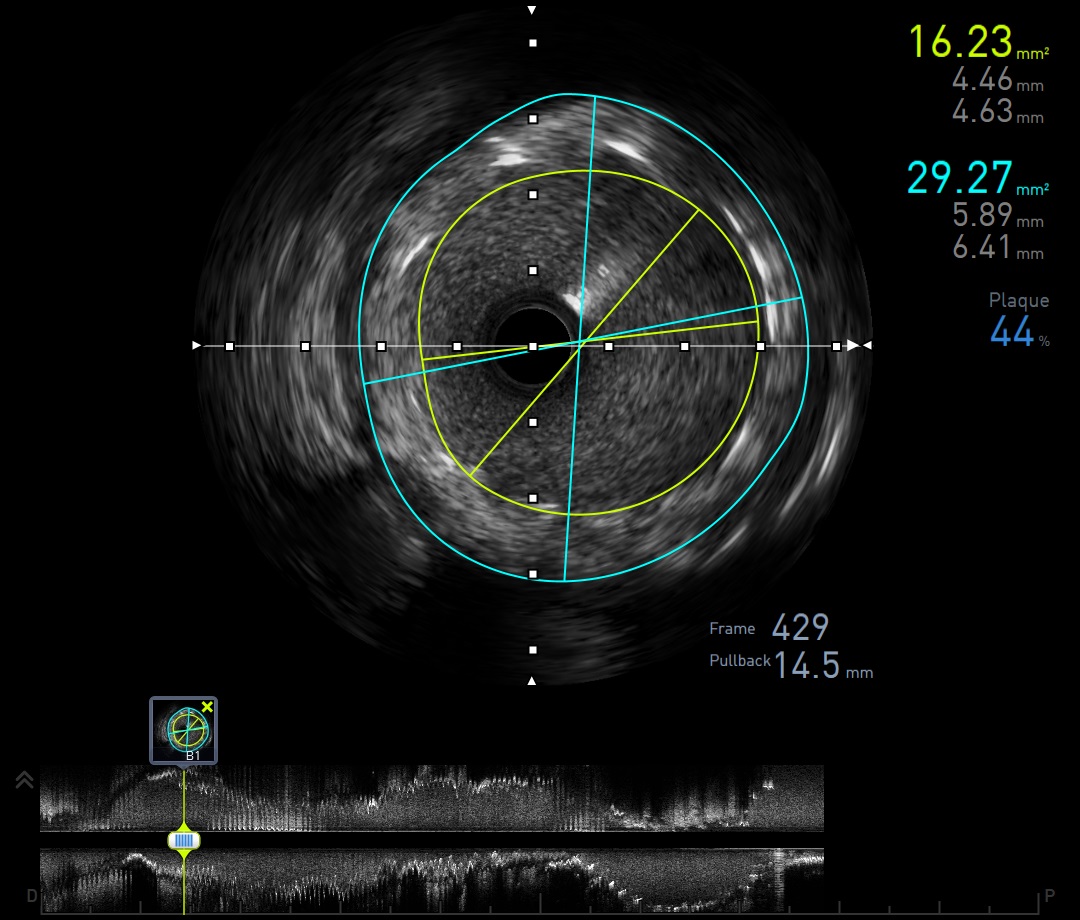
IVUS post
| Segment | MLA (mm2) | Lumen diameter (mm) | Vessel diameter (mm) | Plaque Burden (%) |
| Distal RCA | 16.23 | 4.46/4.63 | 5.89/6.41 | 44 |
| Mid RCA (lesion) | 15.19 | 4.28/4.51 | 5.41/5.78 | 38 |
Well opposed stent, no dissection
Case Summary
Presence of coronary vessel dissection had been considered as a strong contraindication to rotational atherectomy. This mainly due to concern of subintimal delivery of the atherectomy burr and resultant in coronary perforation.
Learning points from this case:
1. Choice of debulking agent: rotational vs orbital atherectomy
2. IVUS guided PCI was used to confirm the dissection part, degree of calcification and guide the selection of stent size
3. Successful PCI to Ectatic RCA with delivery of THREE 4.5 mm stent size from distal to ostial
4. Careful delivery of rotablator 1.75 mm burr at 160,000 rpm was used, avoiding any tendency for the burr to lurch forward preventing propagation of dissection.