
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-008
Presenter
Ahmed Adel Shaheen
Authors
Ahmed Adel Shaheen1
Affiliation
Louran, Egypt1,
View Study Report
TCTAP C-008
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Left Main Artery Thrombus Treated with Drug Eluting Stent
Ahmed Adel Shaheen1
Louran, Egypt1,
Clinical Information
Patient initials or Identifier Number
MRN
Relevant Clinical History and Physical Exam
75y old male known to be diabetic(type2), hypertensive, Heavy smoker and dyslipidemic. Presented by typical chest pain associated with sweeting, and excessive vomiting for 3 hours. In emergency department, patient crushed and his blood pressure became unrecorded. He was promptly transferred to intensive care unit on maximum vasopressors dose. His blood pressure was still unrecorded, however. the patient then has been intubated and kept on mechanical ventilation.
Relevant Test Results Prior to Catheterization
His electrocardiogram showed ST elevation in lead I, AVL, V2-V6 with right bundle branch block and Bedside Echo showed severe anterior, anterolateral, apical and septal hypokinesis and Ejection fraction was 10-15%. His Troponin and lactate were positive but all other labs were normal.
Relevant Catheterization Findings
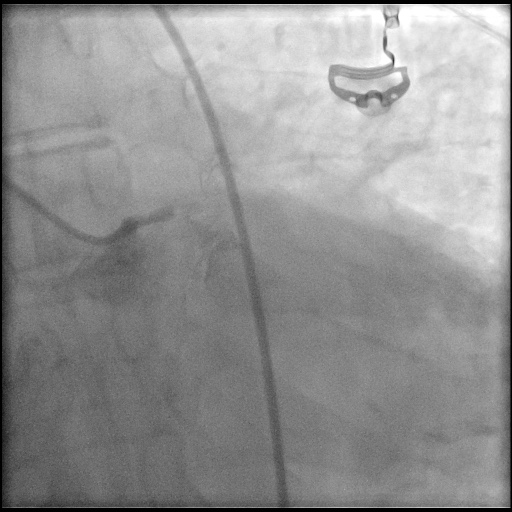
In emergency department; Patient arrested in ventricular fibrillation immediate cardiopulmonary resuscitation was started, thankfully, the patient restored his circulation after 4 cycles. Intensive care unitI activated cathlab around 3.00 am. In cathlab;Coronary angiography through trans-femoral approach showed; 100% left main thrombus occluded lesion.
 LM2.mp4
LM2.mp4
Interventional Management
Procedural Step
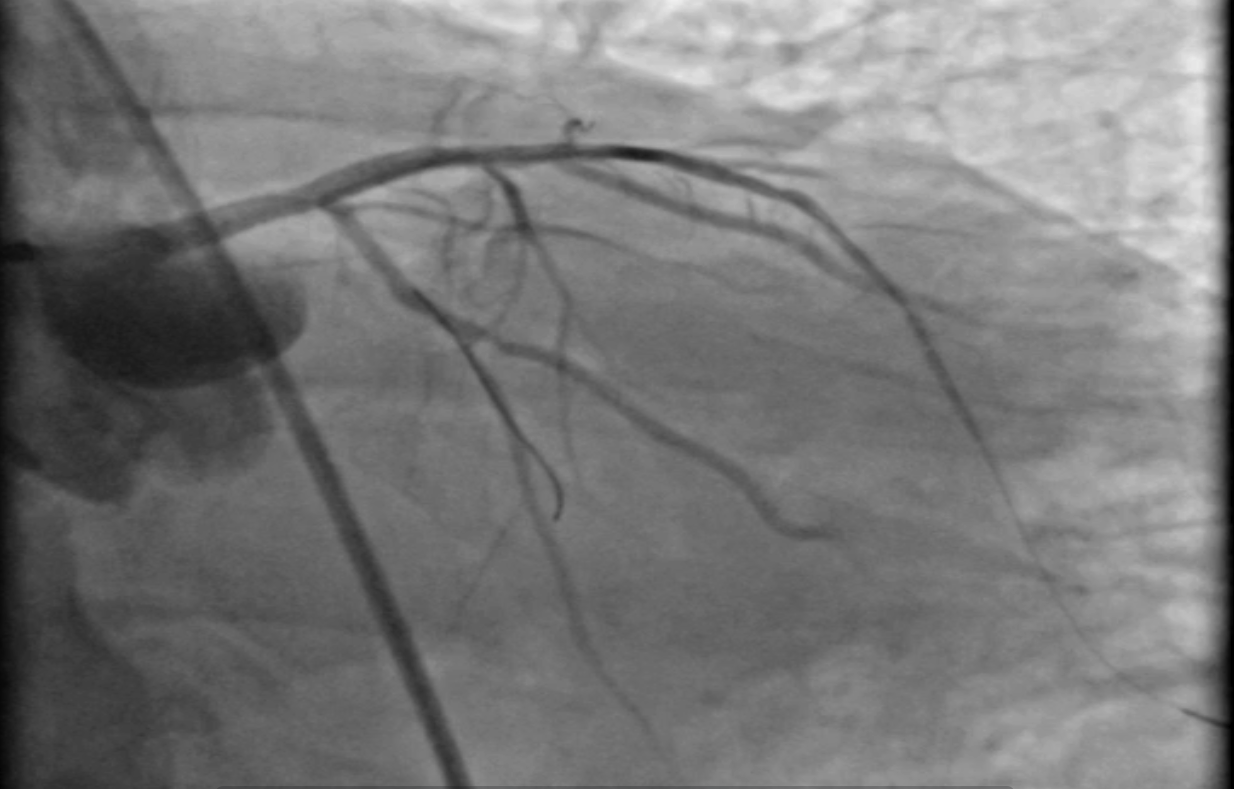
Xtra backup 3.5 mm guiding catheter was engaged into left main coronary artery, then workhorse 0.014 wire was secured distally into ramus intermedius artery. 2.00/15 mm compliant balloon was inflated in the left main artery at 10 atm, Then, wiring both left anterior descending and left circumflex arteries was done using two 0.014 workhorse wires. Then drug eluting stent 3.0/28 mm was deployed from the left main ostium down to the proximal left anterior descending artery. Post dilatation using a non-compliant balloon 3.00/15 mm in left anterior descending artery was done at 16 atm. Finally, proximal optimisation( POT) was done in left main at 20 atm using 3.5/15 mm non-compliant balloon with good final result.

Case Summary
ST-elevation myocardial infarction (STEMI) involving the left main coronary artery (LMCA) has been associated with significant morbidity and mortality. Most studies are limited by small sample sizes. PCI of the ULMCA should be considered as a viable alternative to CABG for selected patients with Ml, including those with ULMCA occlusion and less than Thrombolysis In Myocardial Infarction flow grade 3, cardiogenic shock, persistent ventricular arrhythmias, and significant comorbidities. The higher risk of target vessel revascularization associated with ULMCA PCI compared with CABG is acceptable given the primary need for rapid reperfusion to enhance survival.